Session Information
Session Type: Poster Session D
Session Time: 9:00AM-11:00AM
Background/Purpose: Recent studies have questioned whether CS injections (CSI), a popular treatment recommended by guidelines, hasten progression of knee OA. A recent cohort study suggested a three-fold higher risk for knee OA progression with CSI.
A limitation of such studies is CSI recipients have more advanced knee OA, which is itself a risk factor for OA progression, making it impossible, despite statistical adjustments, to compare those undergoing CSI to those who do not report injections. Patients receiving HA injections (HAI) are a natural comparator to those receiving CSI, as HAI has not been associated with cartilage loss. The purpose of this study was to assess whether CSI was associated with increased rates on knee OA progression in comparison to HAI.
Methods: We used 2 cohort studies of knee OA, MOST and OAI, to look at rates of x-ray progression and total knee replacement (TKR) among CSI or HAI recipients. OAI and MOST visits were performed every 12 and 30 months, respectively, and included knee x-rays and questions about HAI or CSI in the preceding 6 months. The studies use similar acquisition and reading protocols. Kellgren and Lawrence grades (KL) (0-4), joint space narrowing (JSN) (0-3) were scored for both studies and in OAI, medial joint space (JWS250) was measured.
For analysis of x-ray progression, we excluded knees with baseline KL 4, CSI or HAI reported at first visit, and recipients of HAI and CSI. We compared x-rays from the visit before first reported injection to x-rays at the visit after the last injection. TKR without post-injection x-ray was assigned KL grade 4 and JSN 3 at visit at which TKR was first present. Annualized deterioration rates were calculated for KL, JSN and JWS250. Using multivariable linear regression, we examined deterioration rates for reports of injections at single and multiple exams adjusting for age, sex, BMI, study, and baseline KL grade. For TKR survival analysis, we added subjects who reported injections at baseline visits. TKR events were censored after 7 years from first reported injection.
Results: 792 knees were analyzed, of which 647 reported CSI use and 145 reported HAI use. 124 reported CSI and 19 reported HAI at >1 visit. For additional characteristics, see table 1.
Unadjusted analysis for time to TKR is shown in figure 1. The rate of TKR was greater among those with single exam reports of HAI than of CSI (p=.04) but not different for those reporting at multiple exams, although numbers were small. Multivariable analysis showed similar rates of radiographic progression between CSI and HAI among subjects reporting injections at single or multiple exams (table 2).
Conclusion: CSI for knee OA was not associated with higher rate of radiographic progression or progression to TKR than HAI. The risk of disease progression attributed to CSI in earlier studies may reflect the presence of more severe OA in those undergoing injections.
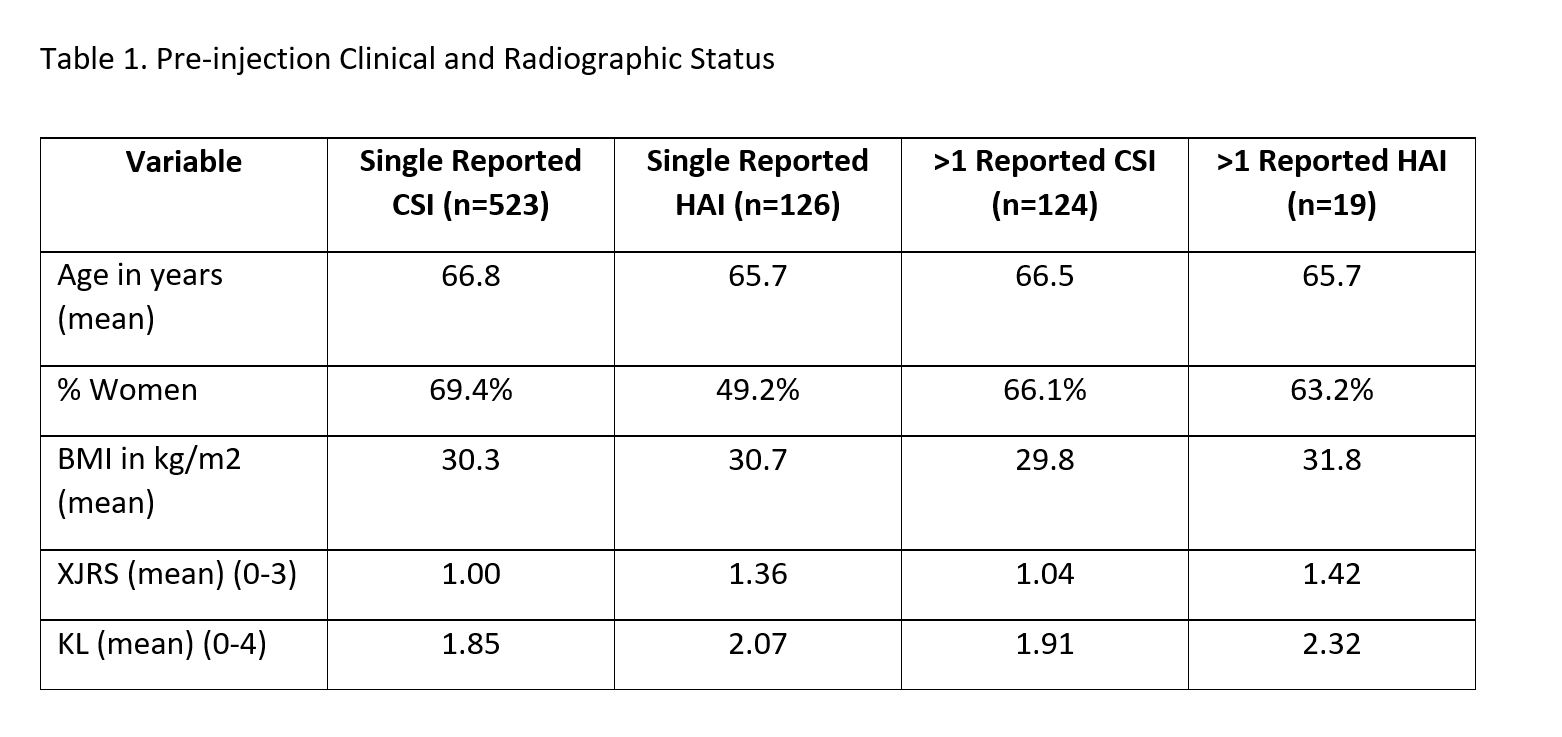 Table 1
Table 1
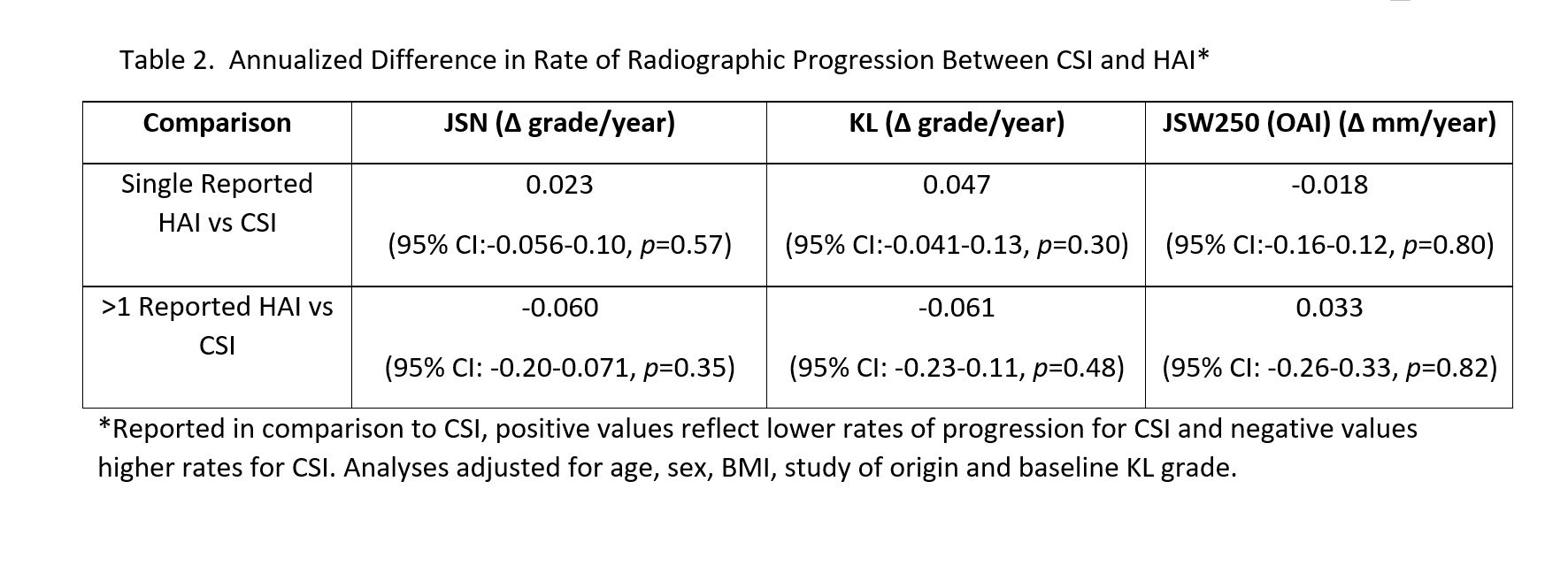 Table 2
Table 2
 Figure 1
Figure 1
To cite this abstract in AMA style:
Bucci J, Chen X, Torner J, Nevitt M, Lewis C, Felson D. Progression of Knee OA with Use of Intra-articular Corticosteroids (CS) vs Hyaluronic Acid (HA) [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/progression-of-knee-oa-with-use-of-intra-articular-corticosteroids-cs-vs-hyaluronic-acid-ha/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/progression-of-knee-oa-with-use-of-intra-articular-corticosteroids-cs-vs-hyaluronic-acid-ha/