Session Information
Date: Sunday, November 13, 2022
Title: Abstracts: Metabolic and Crystal Arthropathies – Basic and Clinical Science
Session Type: Abstract Session
Session Time: 3:00PM-4:30PM
Background/Purpose: Gout patients suffer from an increased burden of cardiovascular disease (CVD). It remains unclear whether this risk is related to an excess of CVD risk factors, unique pathophysiologic mechanisms underlying gout, and/or inadequate gout management. Furthermore, while atherothrombotic CVD event risk has been extensively studied, there is a relative paucity of information on risk of incident heart failure (HF) in gout. Thus, we evaluated the associations of gout and gout treatment status with major adverse cardiovascular events (MACE), HF hospitalization, and CVD-related death in a national cohort of US Veterans.
Methods: We performed a retrospective, matched cohort study in the Veterans Health Administration (VHA) from 1/1999 to 9/2015. Patients with gout (≥2 ICD-9 codes) were matched up to 1:10 on age, sex, and year of VHA enrollment to patients without a gout ICD-9 code or urate lowering therapy (ULT) dispensing. CVD events (overall, fatal and non-fatal MACE, HF hospitalization, HF death) were identified using validated diagnostic and procedure codes in VHA and linked National Death Index data. Among gout patients, gout treatment status was defined in a time-varying manner over 12-month intervals (including a lag to prevent reverse causation) based on adequate serum urate (SU) control (< 6 mg/dL) and ≥2 dispensings of ULT (Mikuls, JAMA Netw Open, 2022). Multivariable Cox regression models adjusting for CVD risk factors were used to examine the associations of gout and gout treatment status with CVD events.
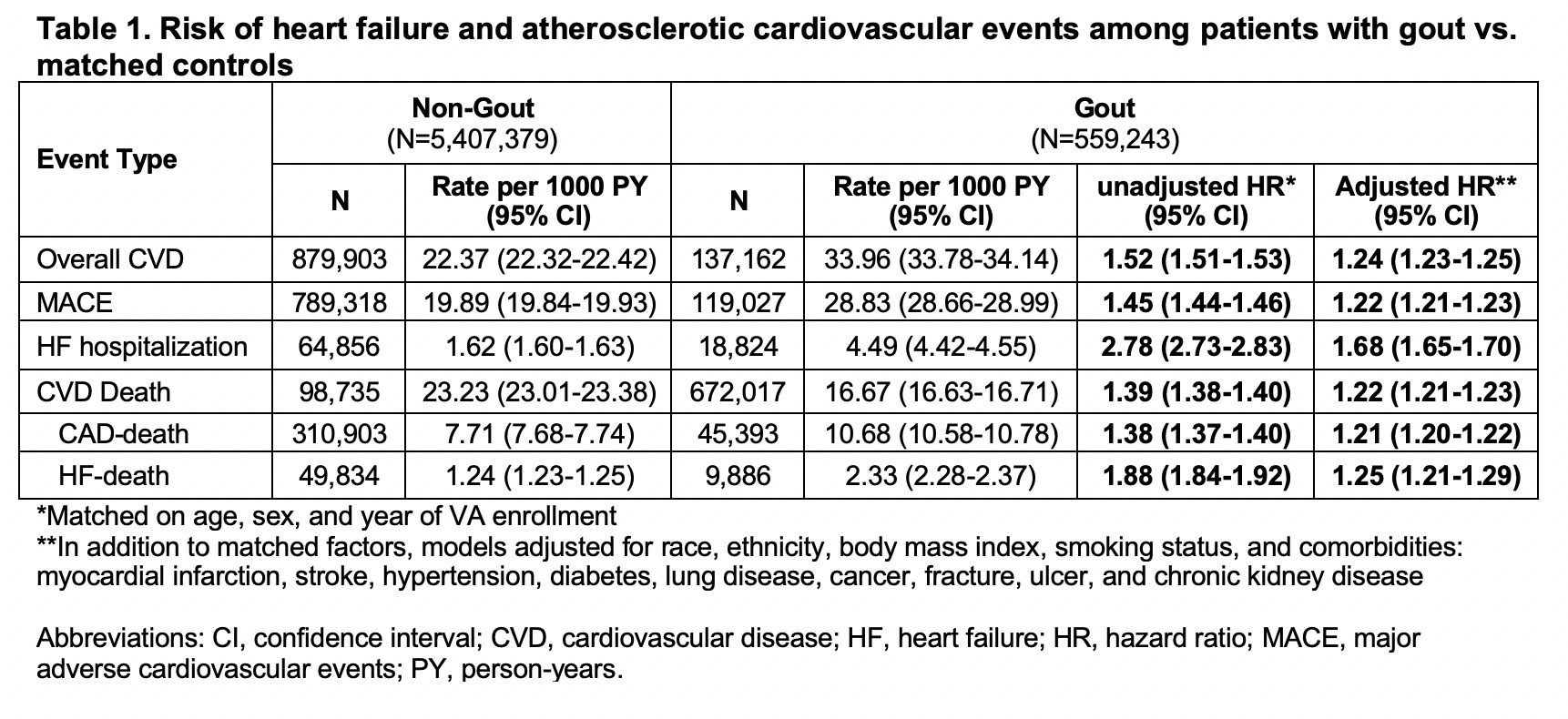
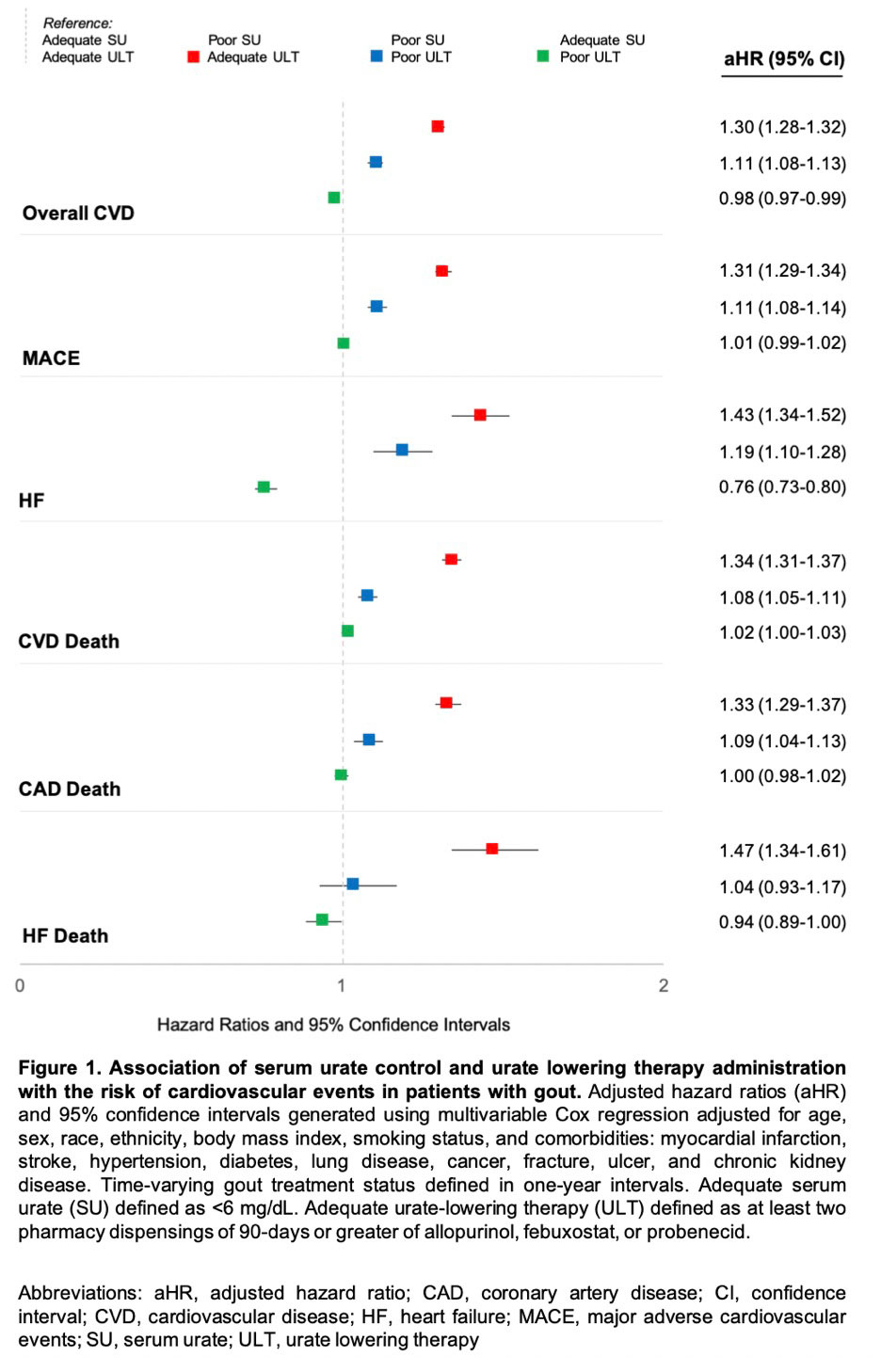
Results: We matched 559,243 gout patients to 5,407,379 non-gout controls (99% male, mean age 67 years). Over 43,331,604 person-years, we observed 137,162 CVD events in gout (IR 33.96 per 1000 PY) vs. 879,903 in non-gout patients (IR 22.37 per 1000 PY). Crude incidence rates of individual CVD events were also higher in gout vs. non-gout (Table 1). Gout was most strongly associated with HF hospitalization, with a nearly 3-fold higher risk (HR 2.78 [2.73-2.83]) that was attenuated but persisted after adjusting for additional CVD risk factors (aHR 1.68 [1.65-1.70]) and excluding patients with prevalent HF (aHR 1.60 [1.57-1.64]). Gout patients were also at higher risk of HF-related death (aHR 1.25 [1.21-1.29]), MACE (aHR 1.22 [1.21-1.23]), and coronary artery disease-related death (aHR 1.21 [1.20-1.22]). Among gout patients, poor SU control was associated with a higher risk of all CVD events, with the highest CVD risk occurring despite receipt of ULT and related to HF hospitalization (aHR 1.43 [1.34-1.52]) and HF-related death (aHR 1.47 [1.34-1.61]) (Figure 1). A 24% lower risk of HF hospitalization was seen in those with controlled SU and poor ULT administration.
Conclusion: In this large, matched cohort study, despite accounting for CVD risk factors, gout was associated with a 68% increased risk of HF hospitalization, 25% increased risk of HF-related death, and a 22% increased risk of MACE. Among gout patients, poorly controlled SU conferred a higher risk of CVD events independent of ULT use, which may represent a surrogate of more severe disease. Continued research investigating a causal link between gout, hyperuricemia, or its treatment, and CVD risk is needed.
To cite this abstract in AMA style:
Johnson T, Helget L, Sayles H, Roul P, O'Dell J, Mikuls T, England B. Poor Serum Urate Control Is a Driver of Excess Cardiovascular Risk in Patients with Gout [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/poor-serum-urate-control-is-a-driver-of-excess-cardiovascular-risk-in-patients-with-gout/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/poor-serum-urate-control-is-a-driver-of-excess-cardiovascular-risk-in-patients-with-gout/