Session Information
Date: Monday, November 9, 2020
Title: SLE – Diagnosis, Manifestations, & Outcomes Poster III: Bench to Bedside
Session Type: Poster Session D
Session Time: 9:00AM-11:00AM
Background/Purpose: There are few predominant African American (AA) epidemiological studies in Cutaneous Lupus Erythematosus (CLE). The Gilliam classification divides CLE into lupus specific, acute cutaneous LE (ACLE), subacute cutaneous lupus (SCLE) and chronic variants (CDLE). Evidence shows SLE can lead to lower vitamin D levels since patients are usually photosensitive and advised to practice sun protection measurements. Also, it is important to consider the probability that vitamin D (Vit. D) deficiency could have a role in the prediction of disease activity given its role on the immune system. The aim of our study was to evaluate the correlation between vitamin D level and disease activity based on laboratory markers, in an AA CLE cohort.
Methods: From Rheumatology and Dermatology clinic at University Medical Center, New Orleans, a total of 182 patients’ charts were retrospectively reviewed from 2015 to 2019. Using ICD-10 codes we cross reference the diagnosis of SLE, DLE, other local LE and SCLE. A total of 67 patients’ data extracted including: age, ethnicity, smoking, ANA, SSA and anti-ds DNA positivity, complement 3 (C3) and complement 4 (C4) levels, Protein/Creatinine ratio (Pr/cr) (< 450 mg/g normal), and Vit. D levels (< 12 ng/ml deficiency). 5 of those patients were excluded since not AA and 4 additional for missing data. In analysis including variable “Pr/cr ratio”, 4 patients had missing data with a total of 54 patients included. Vit. D value was the dependent variable and the remaining were independent variables. For all variables, we calculated frequency and percentage (Table 1). Fisher’s exact test found there was correlation in ANA, SSA, C3, pr/cr ratio in predicting patient’s vitamin D. Only these variables were considered for a stepwise linear regression.
Results: Demographic description in Table 1(mean age: 45 yrs.; female: n=56, male = 11). First, we considered the non-stratified group and excluded pr/cr variable. Assuming equal power for all variables a stepwise linear regression predicted the following variables associated with low Vit D: CD3 value < 80 had a decrease in Vit. D level by 8.3 ng/ml compared with CD3 value > 80 (p < 0.05); SSA positive, associated with decrease of Vit. D by 5.13 ng/ml compared to SSA negative patients (p = 0.05) (Table 2). When data was stratified based SCLE and CCLE (Table 1), only CCLE patients C3 values < 80 had significant association with lower Vit. D by 7.90 ng/ml (p< 0.05) (Table 3). There was not significant predictor for SCLE possibly due to small sample size. Finally, adding pr/cr ratio as independent variable to the whole group, SSA positivity, C3 by association and increase pr/cr ratio are significantly associated with low Vit D. When all variables are considered as equal then we can expect patients with increased pr/cr ratio had a decrease in Vitamin D level of 10.26 ng/ml compared with patients whose values are normal (p < 0.05).
Conclusion: To the best of our knowledge this is the first AA CLE cohort. Our findings showed decreased C3 levels, SSA positivity and increased pr/cr ratio correlate with Vitamin D deficiency. This association was statistically significant and carries a clinically importance given Vitamin D could be used as a surrogate marker for systemic disease activity in AA with CLE.
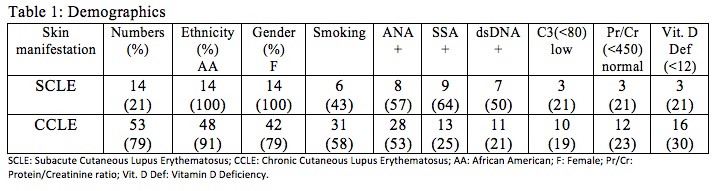 Table 1: Demographics
Table 1: Demographics
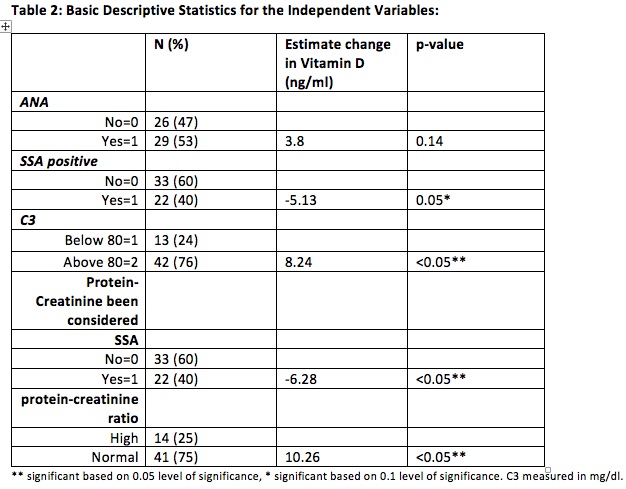 Table 2: Basic Descriptive Statistics for the Independent Variables
Table 2: Basic Descriptive Statistics for the Independent Variables
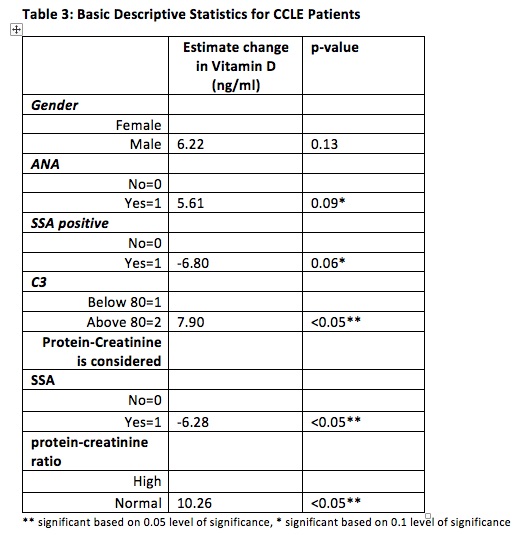 Table 3: Basic Descriptive Statistics for CCLE Patients
Table 3: Basic Descriptive Statistics for CCLE Patients
To cite this abstract in AMA style:
Robledo-Vega I, Scheinuk J, Pardo E, Pratt A, Mahato S, Chapple A, Guevara M. Vitamin D Level: Predictor of SLE Disease Activity in AA Cohort with CLE? [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/vitamin-d-level-predictor-of-sle-disease-activity-in-aa-cohort-with-cle/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/vitamin-d-level-predictor-of-sle-disease-activity-in-aa-cohort-with-cle/