Session Information
Date: Saturday, November 7, 2020
Title: Epidemiology & Public Health Poster II: OA, Osteoporosis, & Other Rheumatic Disease
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Osteoarthritis (OA) and heart disease (HD) are among the most common chronic conditions. Several studies have shown that OA increases the risk of HD later in life, even after adjusting for socioeconomic factors, functional limitations and obesity. Much of the literature considers OA of a specific joint, but there is increasing realization that OA is a multi-joint disease for many, with a greater potential for systemic inflammatory load, a risk factor for HD. Our objective was to compare the burden of HD risk factors between those with and without OA, and consider differences between those with single- and multi-joint OA.
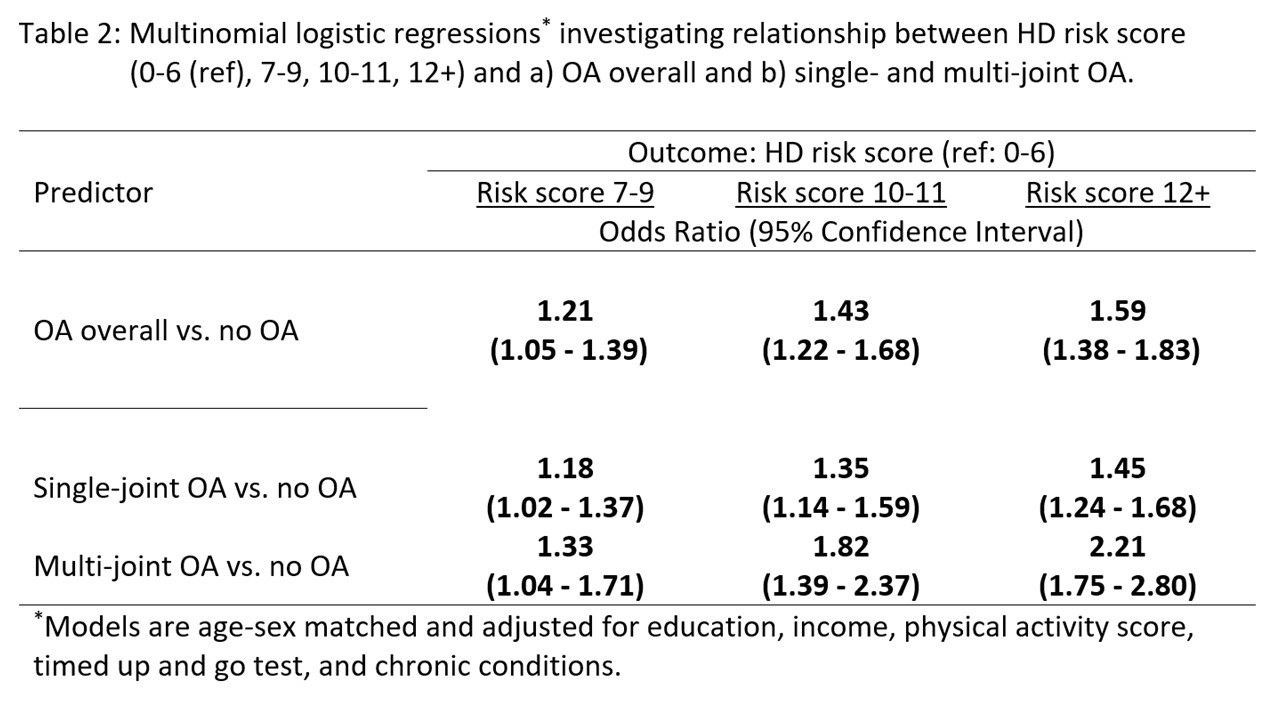
Methods: Data are from cycle 1 of the Canadian Longitudinal Study on Aging, a national study of a representative sample of individuals aged 45-85. Respondents indicated a doctor diagnosis of OA in the knees, hips or hands. Those reporting arthritis other than OA, any form of HD, or use of HD medications were excluded. A 1:1 age and sex non-OA match was randomly selected for every individual with OA. OA was characterized as single or multi-joint OA. HD risk factors: high sensitivity C-reactive protein (hsCRP), high density lipoprotein (HDL), triglycerides, cholesterol, body fat %, body mass index, blood pressure, waist size, Hemoglobin A1c, and smoking history. Each risk factor was scored 0, 1, or 2 using established cut-offs for low/medium/high HD risk, then summed to give an HD risk score and categorized as 0-6, 7-9, 10-11 and 12+ based on quartiles. Covariates: age, sex, education, income, physical activity score, timed up and go functional test and comorbidity count. The association between HD risk score category and a) OA overall and b) single- and multi-joint OA was quantified using multinomial logistic regressions, adjusting for covariates.
Results: The matched sample consisted of 6098 respondents (3049 with OA). The median age was 63 years, 55.8% were female. Several HD risk factors were elevated among those with OA vs. without, including hsCRP, a systemic inflammation marker. Individuals with OA were in the ‘high’ risk category more frequently than non-OA individuals for all but 3 (HDL, cholesterol, and smoking) risk factors. This was reflected in the overall HD risk score: the proportion of OA respondents in the higher score categories was also more frequent for multi- vs. single-joint OA (Table 1). The age-sex matched and covariate adjusted regressions showed that those with OA had significantly greater odds of higher HD risk score than those without OA, with a significant trend of increasing odds for increasing quartile of HD risk score (Table 2). The trend of increasing odds was greater for those with multi-joint than single-joint OA.
Conclusion: Individuals with OA and without HD, and more so those with multi-joint OA, had a worse HD risk profile than individuals without OA. Greater joint involvement and systemic features may be an additional link between OA and HD. Improving overall HD risk-stratification for people with OA is important for enhanced approaches to prevention/intervention. Furthermore, the findings suggest that an exclusive focus on individual joints in OA care and research may limit our ability to effectively manage, treat and understand OA.

To cite this abstract in AMA style:
Perruccio A, Zahid S, Yip C, Power J, Canizares M, Heckman G, Badley E. The Relationship Between Heart Disease Risk Profile and Osteoarthritis, Overall and by Multi-/Single-Joint Involvement [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/the-relationship-between-heart-disease-risk-profile-and-osteoarthritis-overall-and-by-multi-single-joint-involvement/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-relationship-between-heart-disease-risk-profile-and-osteoarthritis-overall-and-by-multi-single-joint-involvement/