Session Information
Date: Sunday, November 8, 2020
Title: RA – Diagnosis, Manifestations, & Outcomes Poster III: Cardiopulmonary Aspects
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Coronary microvascular disease (CMD) is associated with increased mortality in RA independent of traditional cardiovascular (CV) risk factors. Inflammation likely plays an important role the pathogenesis of RA. Studies suggest that higher RA clinical disease activity index (CDAI) is associated with a higher degree of CMD. However, it is not known whether specific inflammatory pathways implicated in RA, including interleukin 6 (IL-6), tumor necrosis factor alpha (TNFα), and interleukin 1 beta (IL-1β), play a stronger role than others in the pathogenesis of CMD in RA. The objective of this study was to identify the associations between inflammatory cytokines and CMD in RA.
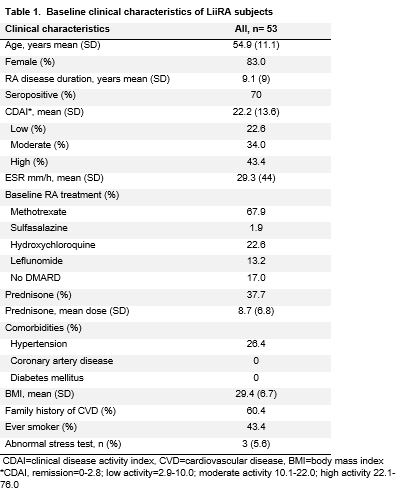
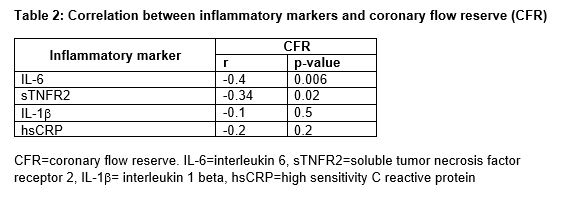
Methods: We used baseline data from the first 53 subjects enrolled in the Lipids, Inflammation, and CV Risk (LiiRA, ClinicalTrials.gov: NCT02714881) study. LiiRA enrolls RA patients, age >35, immediately prior to TNF inhibitor initiation. Exclusion criteria include known cardiovascular disease, statin use, prednisone dose >10mg, or biologic DMARD (bDMARD) use in the past 6 months. All subjects underwent a stress myocardial perfusion PET scan (cardiac PET). The cardiac PET quantifies myocardial blood flow at rest and during maximal hyperemia in response to a coronary vasodilator. Coronary flow reserve (CFR) is the ratio of myocardial blood flow during maximal hyperemia over that at rest. A lower CFR in the absence of obstructive coronary artery disease (CAD) is indicative of CMD. Demographics, RA clinical factors, serum inflammatory markers, and CDAI were collected. Inflammatory markers included high-sensitivity C-reactive protein (hsCRP), IL-6, soluble TNF receptor 2 (sTNFr2), and IL-1β. We tested the association between inflammatory markers and CFR using the Spearman correlation.
Results: The mean age of subjects in LiiRA was 55 years, 83% were female, 70% seropositive, with a mean RA disease duration of 9.1 years (Table 1); per the study protocol, none of the subjects were on a bDMARD. Baseline cardiac risk factors were uncommon; no patients had diabetes and 26 % had hypertension. IL-6 and sTNFR2 were correlated with a lower CFR. However, no significant associations were observed between IL-1β and hsCRP (Table 2).
Conclusion: Among RA patients with no history of overt CAD and low prevalence of CV risk factors, the severity of CMD was correlated with IL-6 and sTNFR2 but not IL-1β or hsCRP, a general measure of inflammation. These findings provide potential insight into the mechanisms by which inflammation mediates microvascular dysfunction.
To cite this abstract in AMA style:
Weber B, He Z, Huang S, Solomon D, Massarotti E, Golnik C, Seyok T, Brownmiller S, Martell L, Barrett L, Bibbo C, Bolster M, DiCarli M, Liao K. Specificity for Inflammatory Pathways Associated with Coronary Microvascular Dysfunction in Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/specificity-for-inflammatory-pathways-associated-with-coronary-microvascular-dysfunction-in-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/specificity-for-inflammatory-pathways-associated-with-coronary-microvascular-dysfunction-in-rheumatoid-arthritis/