Session Information
Session Type: Poster Session B
Session Time: 9:00AM-10:30AM
Background/Purpose: Adipokines are fat and muscle-secreted protein hormones that regulate metabolism. Adiponectin has been associated with fracture in the general population while the role of leptin is less clear. Fibroblast Growth Factor (FGF)-21 is an indicator of metabolic stress has been associated adverse bone morphology and strength in other settings. We assessed whether adipokines are associated with a history of osteoporosis and fracture at time of enrollment in the Veteran’s Affairs Rheumatoid Arthritis (VARA) registry and whether they independently predict future incident fractures.
Methods: Participants were adults with physician-confirmed RA. Adipokines were measured on the MesoScale Discovery platform using banked serum from enrollment. Values were log-adjusted, standardized (per SD), and dichotomized above/below the median value. A history of osteoporosis and fracture were defined based on the presence of any relevant HCUP-CCS codes within the 12 months before enrollment. Incident osteoporotic fracture was defined based on validated algorithms using diagnostic and procedure codes and confirmed by chart review. Linear regression was used to evaluate differences in adipokines among those with a history of osteoporosis or fracture at enrollment. Multivariable Cox proportional hazard models evaluated associations between adipokines and incident fracture adjusting for demographics, smoking, BMI, prednisone use, comorbidity score, disease activity, and any history of osteoporosis and fracture prior to enrollment.
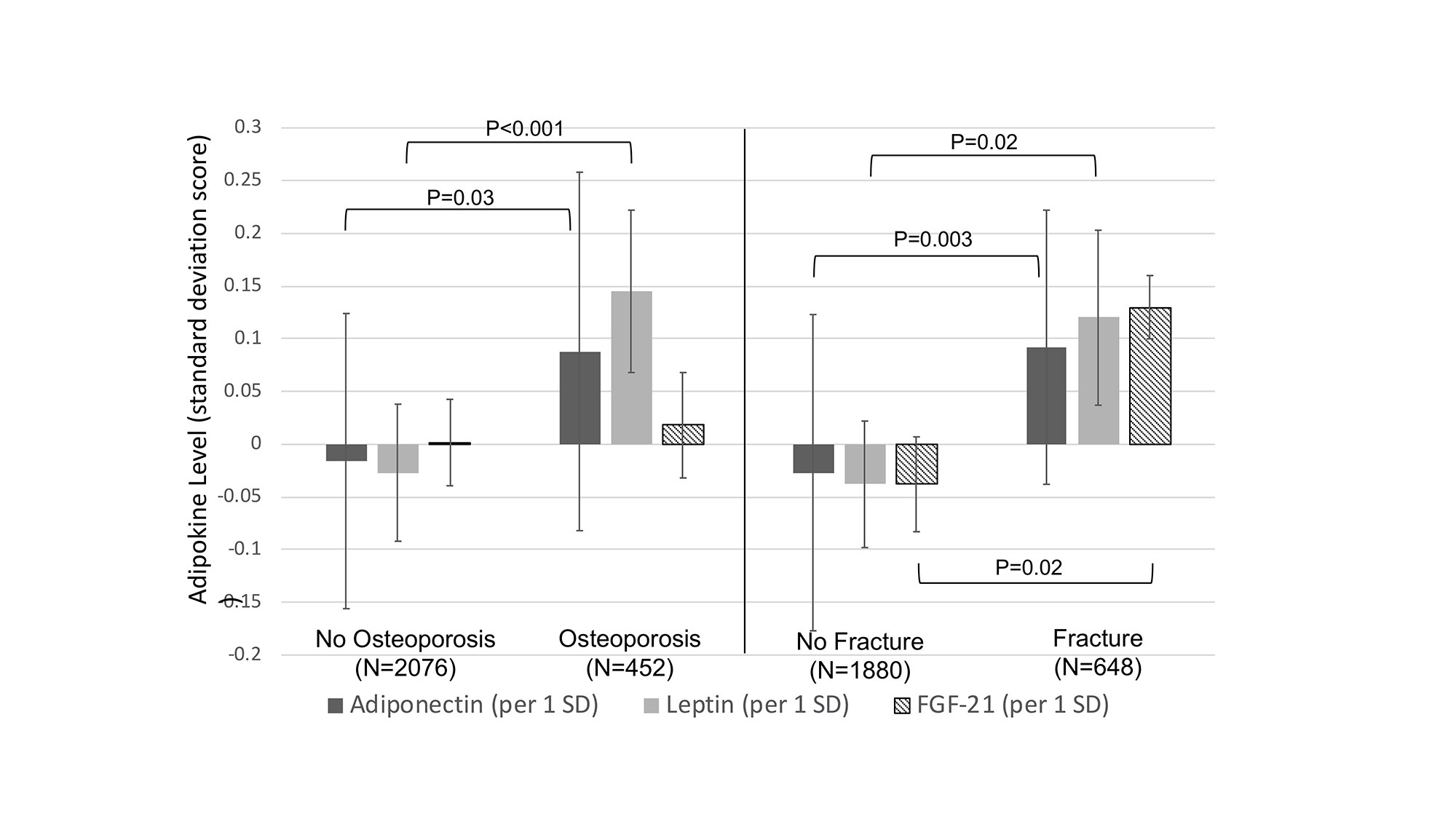
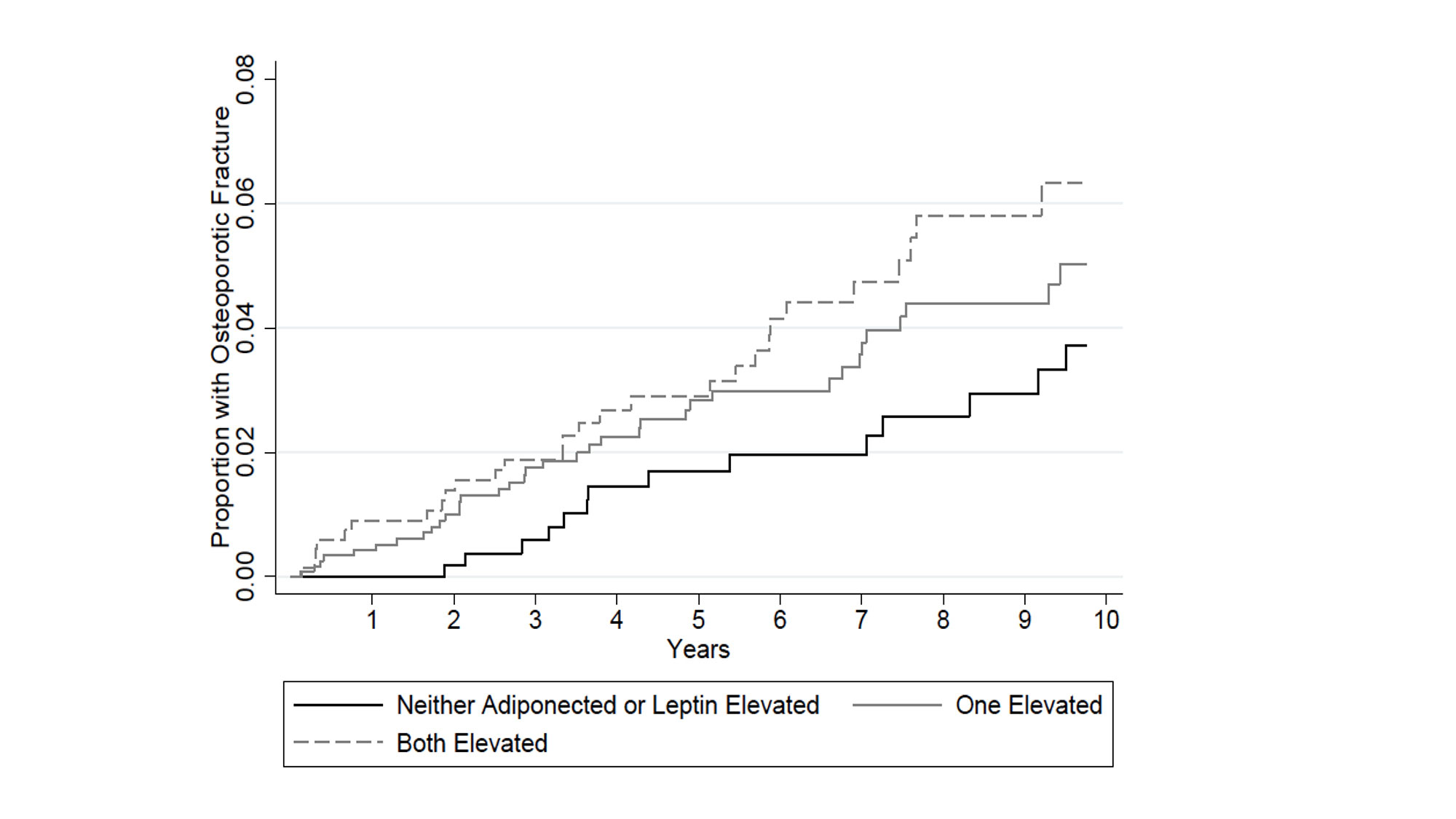
Results: A total of 2512 participants were included (mean (SD) age 71 (10) years; 87% male). At enrollment, 648 patients had a history of any prior fracture and 452 had a history of osteoporosis. Over 16,573 person-years of follow-up, there were 86 incident fractures at a rate of 0.52 per 100 person-years. After adjustment, those with a history of fracture at enrollment had higher adiponectin, leptin, and FGF-21 levels (Figure 1). In addition, those with a history of osteoporosis (with or without prior fracture) had higher levels of adiponectin and leptin. After adjustment, there was a higher risk of incident fracture among patients with adiponectin [HR: 1.43 (1.07, 1.90) p=0.01] and leptin [HR: 1.49 (1.11, 1.98) p=0.006] levels above the median. Patients with elevated levels of both adiponectin and leptin experienced a much higher risk of fracture compared to those in whom neither was elevated [HR: 2.14 (1.38, 3.33) p=0.001] (Figure 2).
Conclusion: Elevations in adipokines are independently associated with a greater prevalence of osteoporosis and fracture at enrollment and predict incident osteoporotic fractures in patients with RA. perhaps by identifying patients who have altered body composition or disrupted metabolic pathways. Further study is needed to determine how alterations in adipokines over time could be leveraged as part of a precision medicine approach with the goal of preventing fracture.
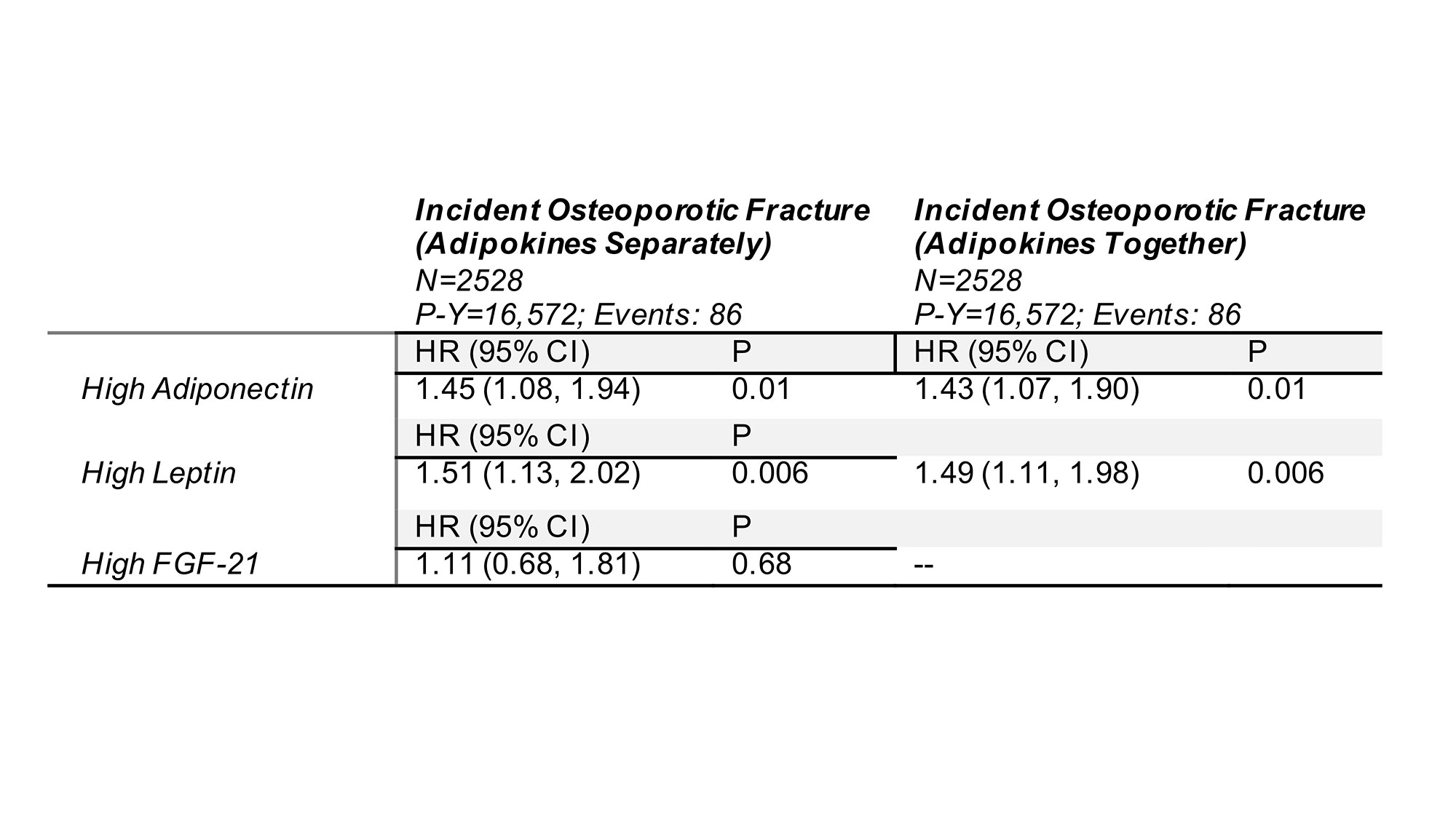
All models adjusted for age, age2, sex, race, BMI, smoking, history of osteoporosis, history of fracture, prior use of bisphosphonates, DAS28, prednisone use, comorbidity score (RDCI), and date of enrollment (and squared term). Note: The RDCI was adjusted down 1 point for those with prevalent fracture.
Abbreviations: P-Y= Person-years; HR= Hazard Ratio; CI= Confidence Interval; BMI= Body Mass Index; TNFi= Tumor Necrosis Factor Inhibitor
To cite this abstract in AMA style:
Baker J, Wysham K, England B, Roul P, Lenert A, Cannon G, Sauer B, Thiele G, Mikuls T. Serum Adipokines Predict Incident Osteoporotic Fracture in Patients with Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/serum-adipokines-predict-incident-osteoporotic-fracture-in-patients-with-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/serum-adipokines-predict-incident-osteoporotic-fracture-in-patients-with-rheumatoid-arthritis/