Session Information
Date: Tuesday, November 9, 2021
Title: Systemic Sclerosis & Related Disorders – Clinical Poster III (1836–1861)
Session Type: Poster Session D
Session Time: 8:30AM-10:30AM
Background/Purpose: Antinuclear antibodies (ANA) are serological markers for the presence of connective tissue diseases [1]. In some patients, a pattern can be detected in ANA immunofluorescence that resembles an anti-dense-fine-speckled-70 antibody (anti-DSF70)[2]. This is detected less frequently in patients with connective tissue diseases (CTD) and is therefore often used as an exclusion criteria for CTD [2]. To date, however, it remains unclear how the presence of an anti-DSF70 reliably rules out CTD. We aimed to investigate the extent to which CTD can be excluded by the presence of anti-DFS70 and whether there are discrepancies between patients with CTD and negative anti-DSF70 and those with CTD and positive anti-DSF70.
Methods: We analyzed data of 460 patients who were tested for the presence of anti-DSF70 at the University Hospital Bonn, Germany. Patients were examined with regard to clinical symptoms and signs, type of rheumatic disease, type of CTD, fulfillment of the classification criteria for the particular CTD, presence of anti-DSF70, other systemic autoantibodies and ANA titers by indirect immunofluorescence (IIF) assays and immunoblots. Gold standard for presence of a CTD was the diagnosis of the treating rheumatologist.
Differences between anti-DSF70 positive patients with CTD and anti-DSF70 negative patients with CTD were examined.
In addition, specificity, sensitivity, and positive predictive value for different ANA titers were calculated.
Results: 182 out of 460 patients (79.8% female) had a CTD. 354 patients (77.0%) were anti-DSF70 negative, 81 (17.6%) anti-DSF70 positive and 25 (5.4%) had a borderline anti-DSF70 result.
21 patients with a positive anti-DSF70 were diagnosed with a CTD, which accounts for 25.9% of all anti-DSF70 positive patients. Concerning age, gender, symptoms, clinical signs and other disease-specific antibodies, no significant differences were found between anti-DSF70-positive patients with CTD and anti-DSF70 negative patients with CTD.
Of the 21 DSF70-positive patients with CTD, 12 (57.1%) were tested for the presence of disease-specific autoantibodies. Specific autoantibodies were detected in all of the tested patients with systemic lupus erythematosus, systemic sclerosis, Sjögren’s syndrome and mixed connective tissue disease.
Anti-DSF70 had a specificity of 86.8%, a sensitivity of 26.9% and a positive predictive value of 68.2% at an ANA titer of ≥1:160, with respect to the absence of a connective tissue disease.
Conclusion: Autoantibodies to DSF70 often occur in CTD patients and are therefore not a valid exclusion criteria for a CTD. We observed no CTD in 68.2% of patients who were tested positive. Thus, the DSF70 test can be helpful in ambiguous situations. The additional exclusion of other autoantibodies may make CTD even less probable.
1. Mahler M, Fritzler MJ. Epitope specificity and significance in systemic autoimmune diseases: Epitope specificity. Ann N Y Acad Sci. 2010
2. Mahler M, Hanly JG, Fritzler MJ. Importance of the dense fine speckled pattern on HEp-2 cells and anti-DFS70 antibodies for the diagnosis of systemic autoimmune diseases. Autoimmun Rev. 2012
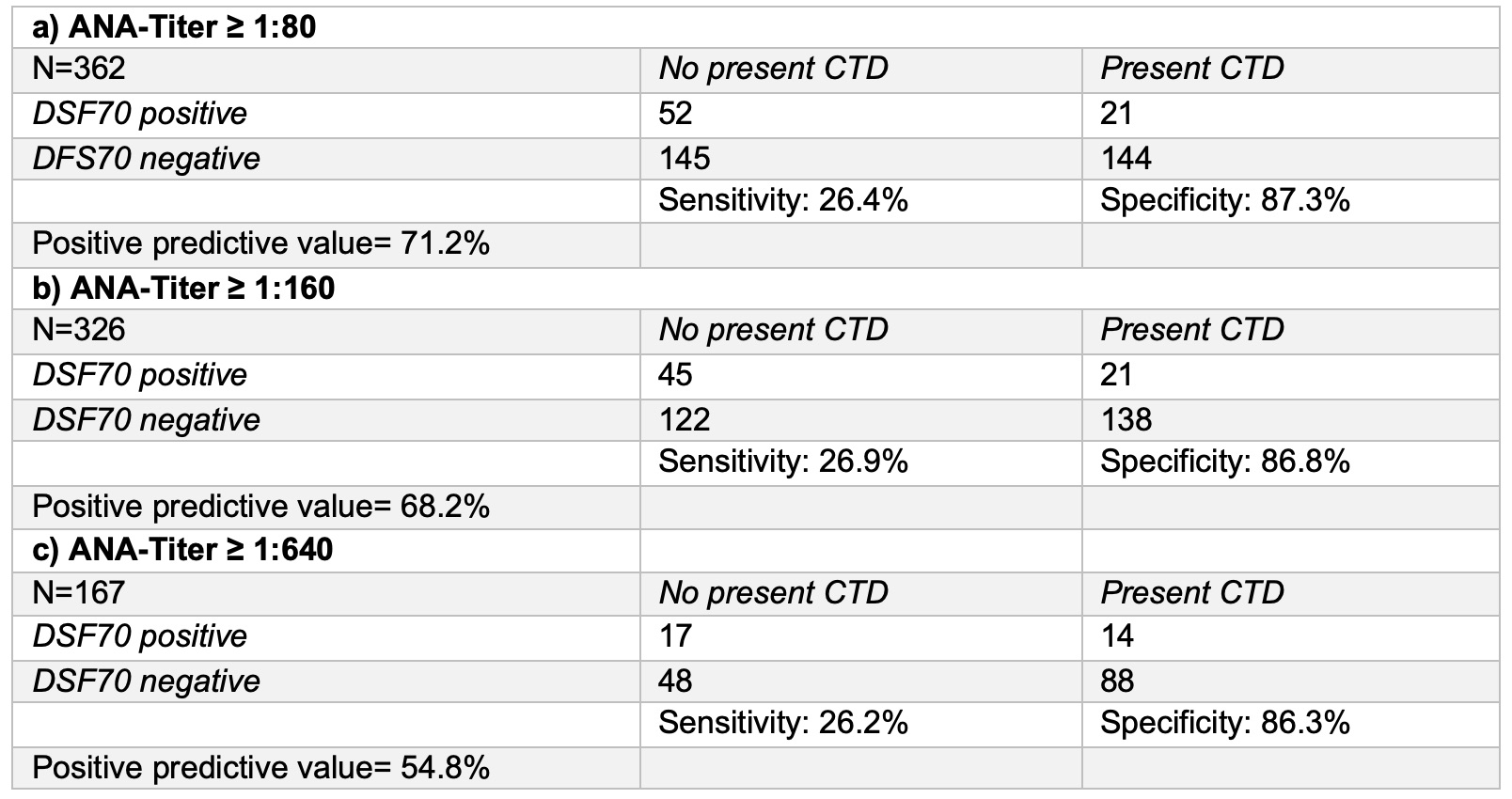 Sensitivity, specificity and positive predictive value of anti-DSF70 autoantibody in different ANA titers (borderline patients excluded)
Sensitivity, specificity and positive predictive value of anti-DSF70 autoantibody in different ANA titers (borderline patients excluded)
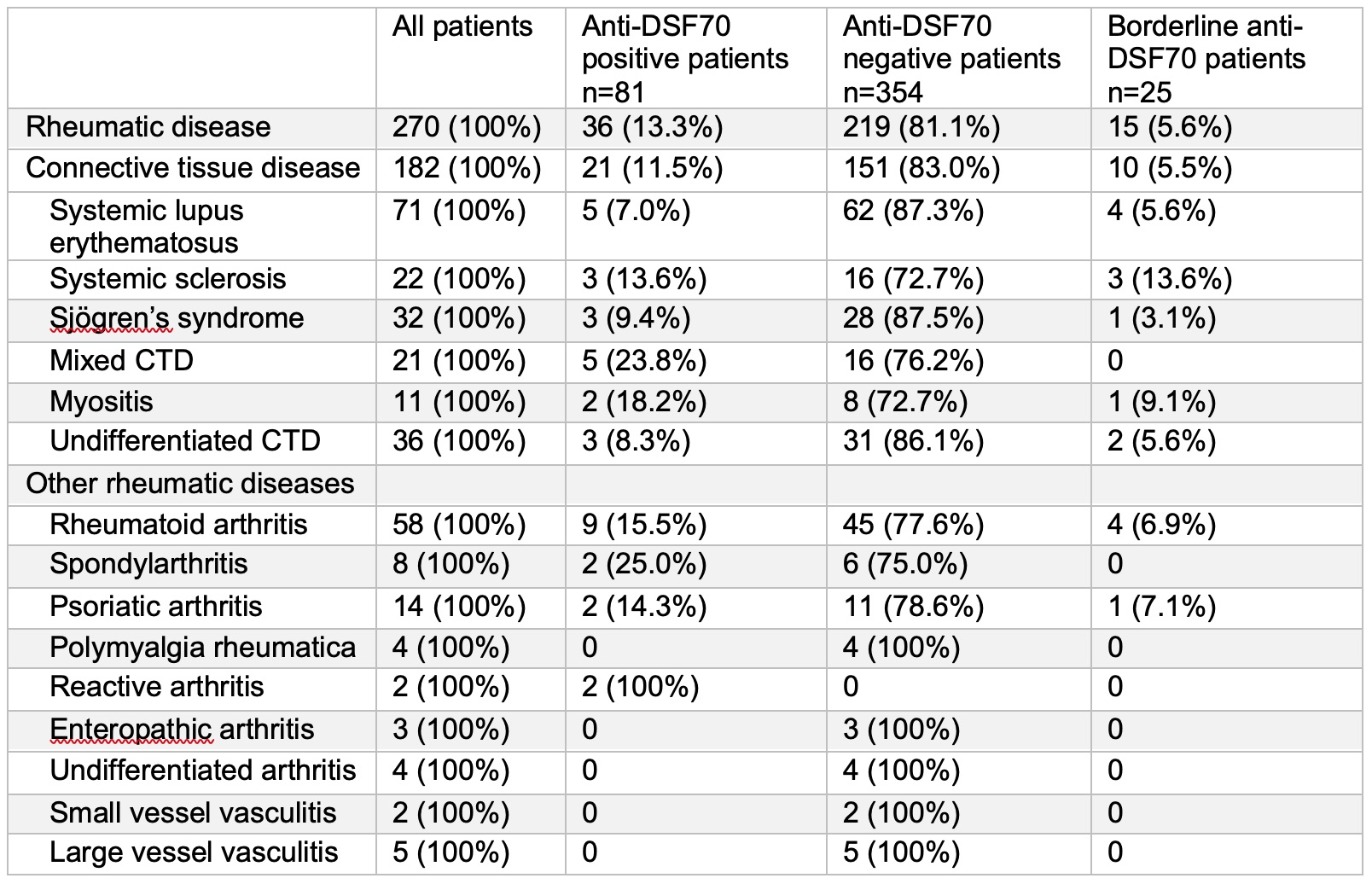 Occurrence of anti-DSF70 in different systemic autoimmune and rheumatic diseases
Occurrence of anti-DSF70 in different systemic autoimmune and rheumatic diseases
To cite this abstract in AMA style:
Mockenhaupt L, Dolscheid-Pommerich R, Behning C, Stoffel-Wagner B, Brossart P, Schäfer V. Presence of Autoantibodies to Dense-Fine-Speckled 70 (DFS70) Do Not Necessarily Rule out Connective Tissue Diseases [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/presence-of-autoantibodies-to-dense-fine-speckled-70-dfs70-do-not-necessarily-rule-out-connective-tissue-diseases/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/presence-of-autoantibodies-to-dense-fine-speckled-70-dfs70-do-not-necessarily-rule-out-connective-tissue-diseases/