Session Information
Date: Sunday, November 12, 2023
Title: (0543–0581) SLE – Diagnosis, Manifestations, & Outcomes Poster I
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: The management of a positive anti-nuclear antibody (ANA) is one of the most common consultations in rheumatology outpatient practice. The prevalence of a positive ANA in the general population is far greater than that of connective tissue diseases (CTDs), including systemic lupus erythematosus (SLE). There are no guidelines on management of a positive ANA without a clear diagnosis. This study seeks to understand how rheumatologists navigate such scenarios.
Methods: We reached out to 40 practicing rheumatologists using an anonymized, case-based survey using multiple choice questions with branching logic. Demographic information was obtained. We used American College of Rheumatology/European Alliance of Associations for Rheumatology (ACR/EULAR) criteria for SLE to design the cases.
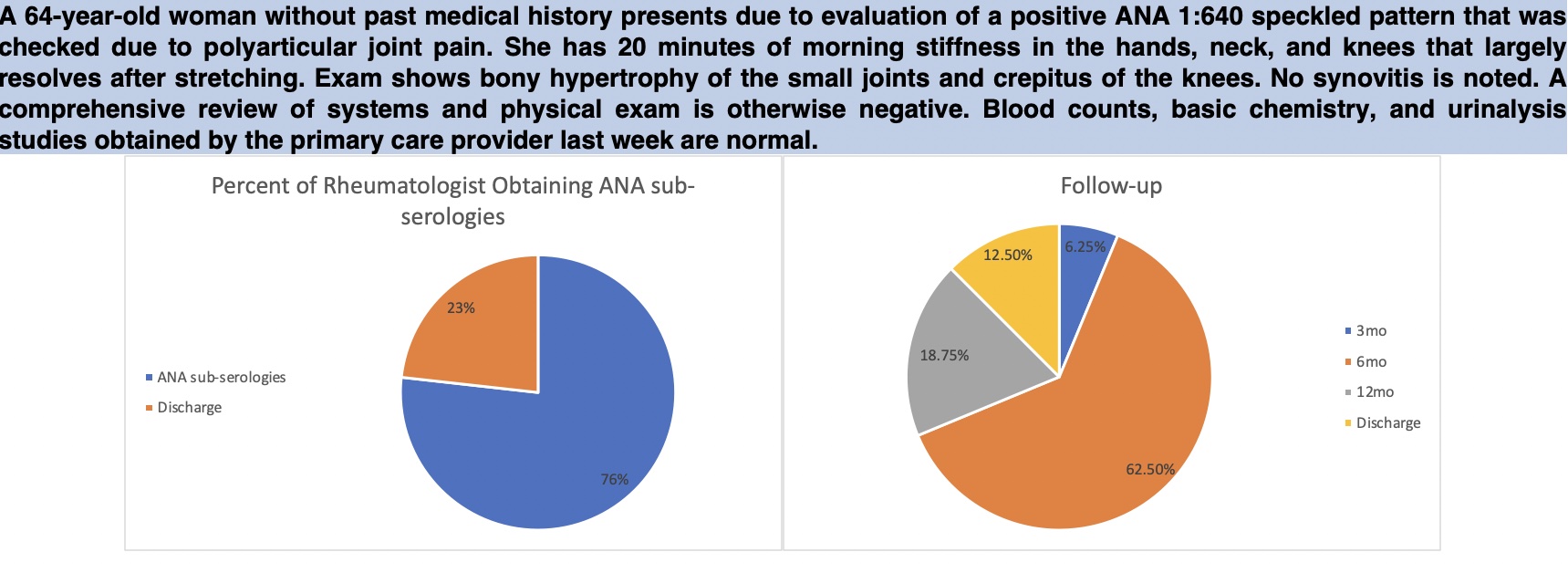
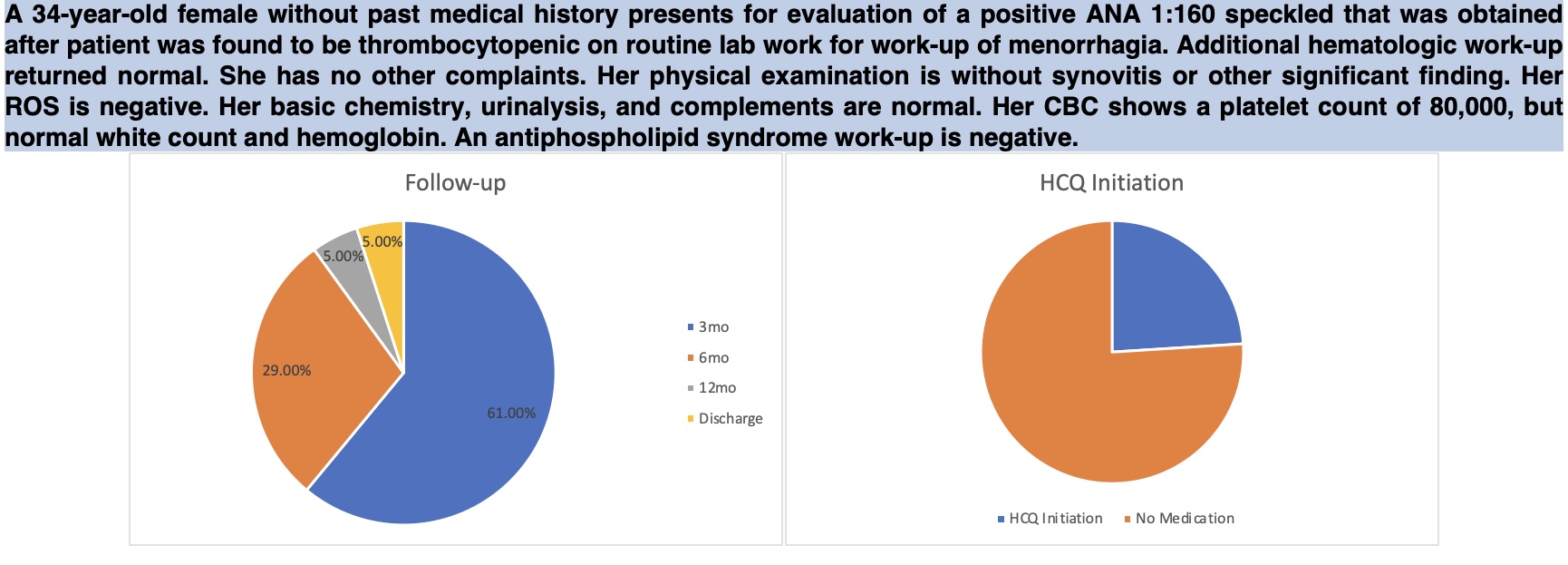
In two cases, patients had a high titer ANA but met no ACR/EULAR criteria for SLE. These cases represent a false-positive ANA (FP-ANA). Two additional cases had patients with low-positive ANA titers, morning-dominant joint stiffness for one hour with a normal musculoskeletal exam, and one ACR/EULAR criteria for SLE. These two cases represent undifferentiated connective tissue disease (UCTD). A final case had isolated thrombocytopenia along with a positive ANA (ITP-UCTD).
Participants were asked if they would obtain ANA sub-serologies or discharge the patient from practice. Of those obtaining sub-serologies, they were asked when follow-up should be arranged, if routine labs are to be obtained at follow-up, and if they would start hydroxychloroquine (HCQ). In each case if sub-serologies were requested, they always returned negative.
Results: 21 out of 40 rheumatologists participated. Work setting: 47% academic, 53% non-academic. Years in practice: 52% with 1-10 years, 24% with 10-20 years, and 24% with more than 20 years. 57% of participants worked in suburban areas. Practice characteristics were not significant in case decision-making.
A mean of 81% of participants in the FP-ANA cases obtained sub-serologies, while the rest chose to discharge the patient without further work-up. Despite negative sub-serologies, 87.5% of participants wished to continue to follow up. One of these cases is detailed in Figure 1.
In all three UCTD cases, all participants obtained sub-serologies. A mean of 55% of participants started HCQ. All participants chose to follow the patient long-term. The ITP-UCTD case is detailed in Figure 2.
Conclusion: Our study suggests that there is substantial variability in how rheumatologists manage the “false-positive ANA” and UCTD. Based on the data, many participants obtain ANA-specific antibodies for a high-titer ANA even when no clinical criteria are met. Most rheumatologists would continue to follow all patients with a positive ANA, although the decision to start HCQ was variable among responders in the cases. Yet, clinical practice guidelines on these practices are lacking. Balancing the economic costs of continued follow up visits and lab testing in these cases with the risk of developing a defined CTD is a complicated endeavor for most rheumatologists. Further studies and evidence are needed to guide decision making in such scenarios.
To cite this abstract in AMA style:
Gupta N, Ford S, Scheiber L, Rao T, Nandan A. Evaluation and Management of the “False Positive” ANA and Undifferentiated Connective Tissue Disease Amongst Rheumatologists [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/evaluation-and-management-of-the-false-positive-ana-and-undifferentiated-connective-tissue-disease-amongst-rheumatologists/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/evaluation-and-management-of-the-false-positive-ana-and-undifferentiated-connective-tissue-disease-amongst-rheumatologists/