Session Information
Session Type: Poster Session A
Session Time: 8:30AM-10:30AM
Background/Purpose: Intra-articular corticosteroids (IACS) are commonly used for symptom management in knee osteoarthritis (KOA) patients, despite the fact that many patients do not respond to this treatment. Knee inflammation (synovitis) is increasingly appreciated as an important factor in OA disease progression and pain, yet studies have failed to find any features of inflammation measured by ultrasound (US) that are associated with pain/function response. Our objective is to test whether nuanced features of sonographically-detected inflammation including synovial tissue quality and synovial vascularity are associated with response after IACS.
Methods: KOA patients presenting to a rheumatology center for regular follow up and steroid injection were administered a standardized US and completed patient surveys prior to injection. Using random-effects linear and logistic models, baseline US features were tested for association with improvement in pain, function, patient-reported global assessment (PGA) of disease activity, and OARSI-OMERACT-defined responder status 18-28 days after IACS injection.
Results: Individuals with echogenic synovium and positive Power Doppler (PD) signal have an improved response to pain (β= 14.500 & 7.655, respectively) and function (β= 11.677 & β= 7.650, respectively) after IACS. Patients with metabolic syndrome have as much as a 30% reduced response to IACS as measured by PGA of disease activity. Only baseline pain (OR= 1.042) and radiographic severity (OR= 5.282) were associated with OARSI-OMERACT-defined response.
Conclusion: Inflammation is not homogeneous across KOA patients, and response to IACS injections depends on baseline symptoms, the phenotype of synovitis, the presence of blood flow within synovium, and baseline radiographic severity.

SD- standard deviation; WOMAC- Western Ontario and McMaster Universities Osteoarthritis Index; PGA- Patient Global Assessment rated by visual analogue scale 0_100; KL Grade- Kellgren-Lawrence Grade; ametabolic syndrome defined by the presence of at least 3 of: i) abdominal obesity waist circumference >102 cm in males and >88 cm in females ii) elevated triglycerides >1.7 mmol/L or medication for hypertriglyceridemia iii) Reduced HDL-C <1.0 mmol/L in males and <1.3 mmol/L in females or medication for reduced HDL-C iv) elevated blood pressure >130 mmHg systolic and/or >85mmHg diastolic or antihypertensive drug treatment in a patient with a history of hypertension v) elevated fasting plasma glucose >5.6 mmol/L or medication for hyperglycemia or A1c >6.5%.
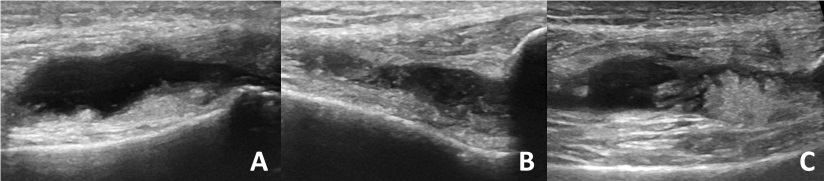
A: Type A synovitis is characterized by a synovial volume predominantly composed of anechoic material (synovial fluid). Little to no circumferential synovial thickening is seen. B: Type B synovitis includes a significant intra-articular abnormal solid component of inflamed synovium which is primarily characterized by low-level echoes. C: In Type C synovitis, inflammation is accompanied by a significant intra-articular solid component of synovium characterized by high level echoes with or without nodular appearance (fronding).
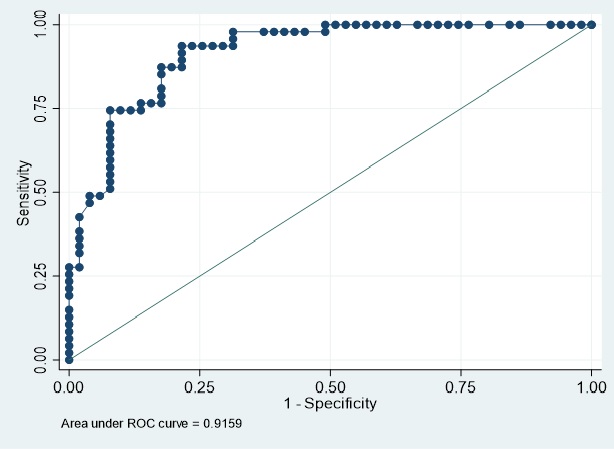
Baseline WOMAC pain and radiographic severity defined as KL grade 3 or 4 (model 1) discriminate between OARSI-OMERACT response with an AUC of 0.9159. With a cut-off probability of P(y)=0.5964, 83.67% of patients are correctly classified into responders or non-responders (sensitivity 74.47% specificity 92.16%).
To cite this abstract in AMA style:
Dima R, Birmingham T, Pinto R, Philpott H, Carter M, Appleton T. Echogenic and Hypervascular Synovium Detected on Ultrasound Are Predictive of a Favorable Response After Intra-articular Corticosteroid Injection in Patients with Knee Osteoarthritis [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/echogenic-and-hypervascular-synovium-detected-on-ultrasound-are-predictive-of-a-favorable-response-after-intra-articular-corticosteroid-injection-in-patients-with-knee-osteoarthritis/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/echogenic-and-hypervascular-synovium-detected-on-ultrasound-are-predictive-of-a-favorable-response-after-intra-articular-corticosteroid-injection-in-patients-with-knee-osteoarthritis/