Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Knee osteoarthritis (OA) is a leading cause of functional limitation in older adults, and stair climbing difficulty is often the first-reported limitation. Previous work has shown that difficulty with stair climbing is associated with future poor health outcomes, including receiving a knee replacement and all-cause mortality. However, the causes of stair climbing difficulty are unclear, creating challenges for appropriate intervention. Lower extremity weakness and knee pain are related to slow gait speed and patient-reported functional limitation, however their relation to stair climbing is not known. Therefore, the purpose of this study was to examine the relation of knee extensor strength and knee pain with incident stair climbing difficulty over 8 years in adults with or at high risk for knee OA.
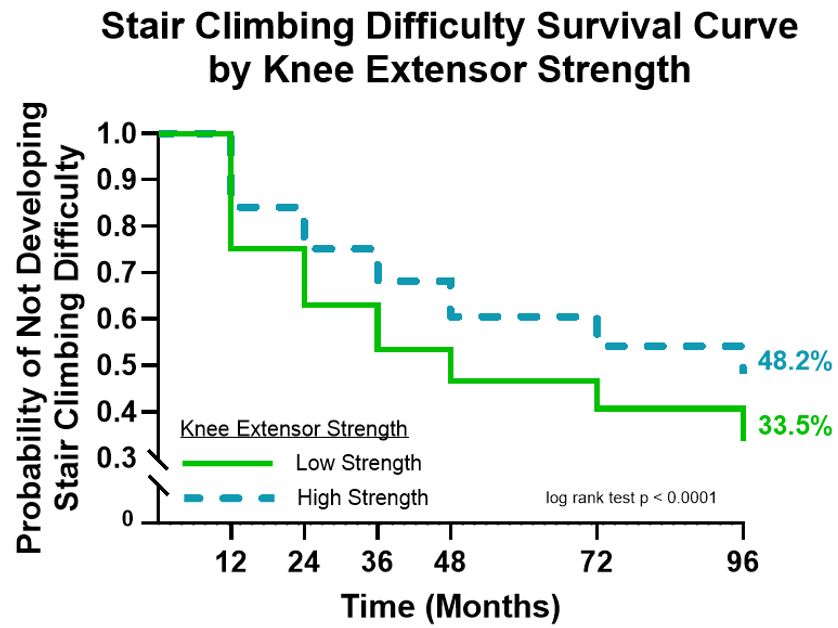
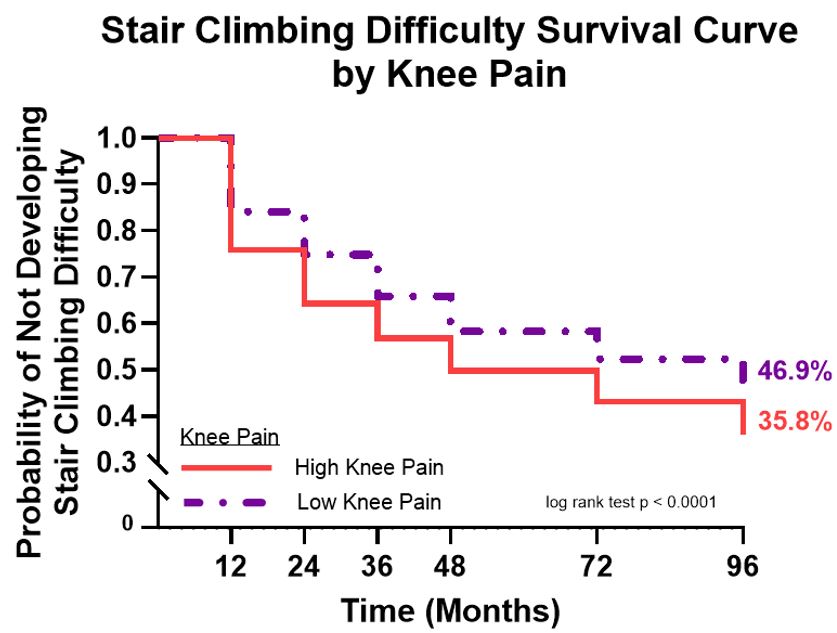
Methods: Data were from the Osteoarthritis Initiative (OAI). Knee extensor strength was defined as maximal isometric knee extensor force from a seated position, collected at baseline (BL). Participants were dichotomized into either a high- or low-strength group based on sex-specific means normalized by body mass index (BMI) [Male: 16.21 N/kg/m2, Female: 10.82 N/kg/m2]. Knee pain was measured on an 11-point visual analog scale (VAS, 0-10) over the last 30 days, collected at BL. Participants were dichotomized into either a high- or low-pain group based on the patient acceptable symptom state (PASS) cutoff of 3/10. Stair climbing difficulty was assessed with the question “Does your health now limit you in climbing several flights of stairs?”. Answer choices included: “Yes, limited a lot”; “Yes, limited a little”; “No, not limited at all.” Stair climbing difficulty was collected at BL, 12-, 24-, 36-, 48-, 72-, and 96-month follow-up. Participants free of difficulty at BL were followed for 8 years to determine if they developed difficulty with stairs. We produced Kaplan-Meier survival curves for cumulative incidence of stair climbing difficulty and used Cox proportional hazards regression to calculate hazard ratios (HR) and 95% confidence intervals (95% CI), adjusted for age, sex, BMI, race, radiographic knee OA, VAS pain, and presence of comorbidity.
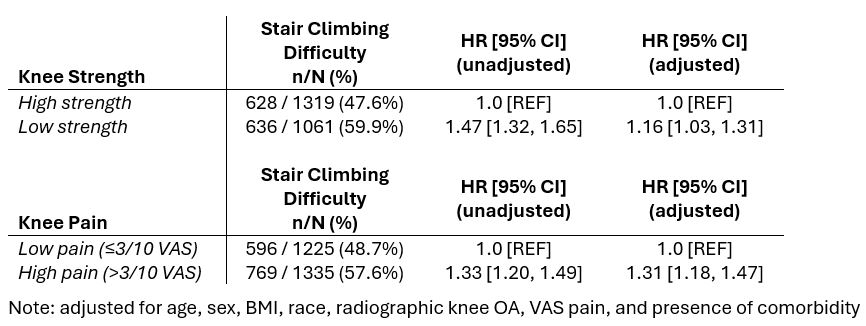
Results: 2380 participants (mean age = 61.2 years old, 52.1% female, mean BMI = 27.7 kg/m2) were included in strength sample. 2560 participants (mean age = 61.1 years old, 52.5% female, mean BMI = 27.7 kg/m2) were included in pain sample. 1264 participants in the strength sample and 1365 participants in the pain sample developed stair climbing difficulty during follow-up (Figure 1, 2). Compared to those with high strength, those with low knee extensor strength had a 16% greater hazard of incident stair climbing difficulty (Table 1). Compared to those with low pain, those with pain above a PASS had a 31% greater hazard of incident stair climbing difficulty (Table 1).
Conclusion: Adults with or at high risk for knee OA who have low knee extensor strength or high pain are at greater risk for developing stair climbing difficulty. These results serve as a first look at why stair climbing difficulty is associated with future functional decline and other important OA-related health outcomes.
To cite this abstract in AMA style:
Jakiela J, Golightly Y, Liles S, Foxworth J, White D. Do Knee Strength and Pain Relate to Developing Stair Climbing Difficulty for Knee Osteoarthritis? [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/do-knee-strength-and-pain-relate-to-developing-stair-climbing-difficulty-for-knee-osteoarthritis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/do-knee-strength-and-pain-relate-to-developing-stair-climbing-difficulty-for-knee-osteoarthritis/