Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Down syndrome (DS), a disorder caused by triplication of chromosome 21, affects around 1 in 1000 births making it one of the most common chromosomal conditions. There is a four-to-six-fold higher risk of autoimmunity in DS compared to the general population. Individuals with DS have a significantly higher prevalence of inflammatory arthritis, termed Down Syndrome-associated arthritis (DA), compared to the general population. Historically, when compared to juvenile idiopathic arthritis (JIA), there has been a delay in diagnosis of DA. Additional research is needed to better elucidate the similarities and differences between DA and JIA, to improve the care of individuals with DA, and allow for earlier diagnosis and treatment. The objective of this study was to compare the clinical presentation and outcomes between DA and JIA in the Pediatric Rheumatology Care & Outcomes Improvement Network (PR-COIN) registry.
Methods: A retrospective case-control study that compared patients with DA matched to patients with JIA using the PR-COIN registry was conducted. Patients were matched on age, gender, arthritis subtype, and medication exposure. Pain rating and clinical juvenile arthritis disease activity scores ([cJADAS], a composite measure of active joint count, physician and patient global assessments [MD-global, Pt-global]), were compared between DA and JIA groups.
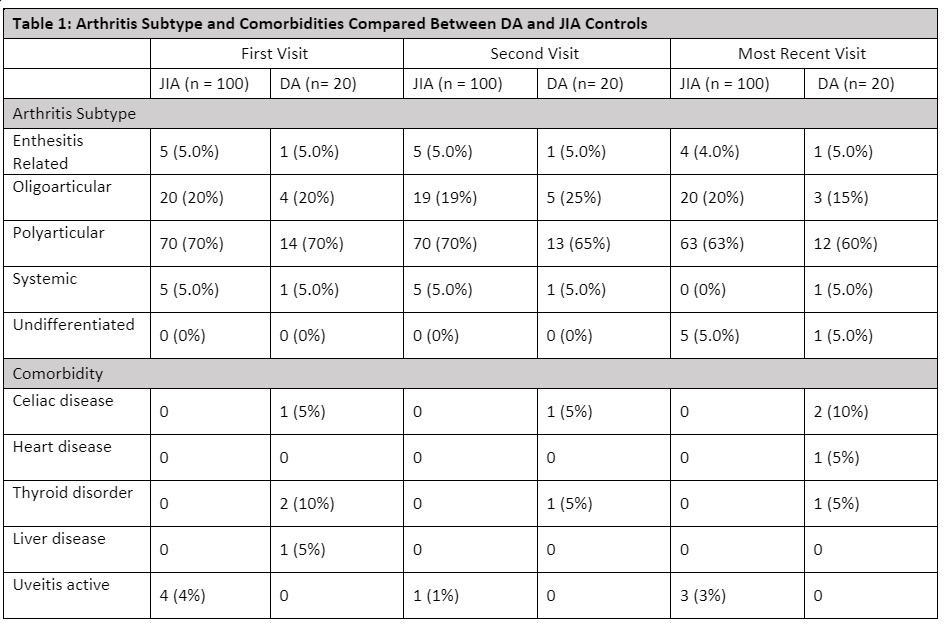
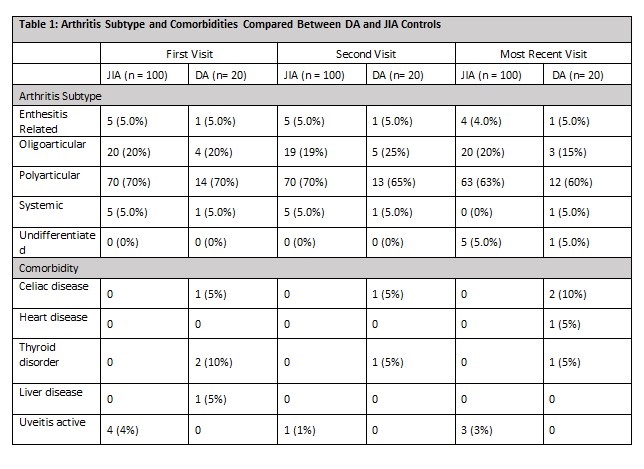
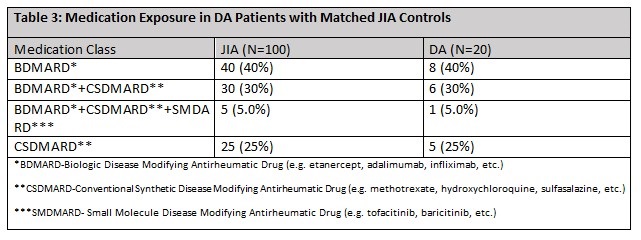
Results: Twenty patients with DA were matched to 100 with JIA. The mean days between first and last visits were 1157 for patients with JIA and 1664 for DA. Patients mostly had polyarticular arthritis subtype (70%), and those with DA had more comorbid autoimmune conditions, but less uveitis compared to the JIA group (Table 1). At the last visit those with DA had lower cJADAS scores compared to the JIA group (1.8 vs 3.9, p< 0.05). All measures of the cJADAS were decreased with the largest decrease in Pt-global scores when comparing between DA and JIA groups (1.1 vs 2.1, p< 0.05). The DA group had an average pain score that improved over time and trended with MD-global score. In comparison the JIA group had a pain score that increased over time and did not trend with MD-global score (Table 2). The medication distribution and exposure were the same between groups (Table 3).
Conclusion: While a delay in diagnosis of DA is not uncommon, this study suggests that with appropriate treatment patients with DA can have improved clinical outcomes compared to those with JIA. Those with DA report less pain compared to those with JIA, and reported pain tracked with active disease for those with DA, but not JIA. This suggests that with appropriate treatment patients with DA demonstrate good resilience and improved clinical outcomes. Further, pain rating may be a poor outcome measure for active disease in patients with JIA and may represent a larger impact of central nervous system sensitization and mental health comorbidities compared to patients with DA. This illustrates the importance of early disease recognition and treatment, which can improve outcomes for those with DA. More research is needed to determine differences in pain perception between those with JIA and DA and understand the clinical significance of this difference in pain perception.
To cite this abstract in AMA style:
Chern I, Singleton J, Wang X, Jones J. Differences in Clinical Presentation and Outcomes Between Down Syndrome-Associated Arthritis and Juvenile Idiopathic Arthritis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/differences-in-clinical-presentation-and-outcomes-between-down-syndrome-associated-arthritis-and-juvenile-idiopathic-arthritis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/differences-in-clinical-presentation-and-outcomes-between-down-syndrome-associated-arthritis-and-juvenile-idiopathic-arthritis/