Session Information
Session Type: Poster Session B
Session Time: 9:00AM-10:30AM
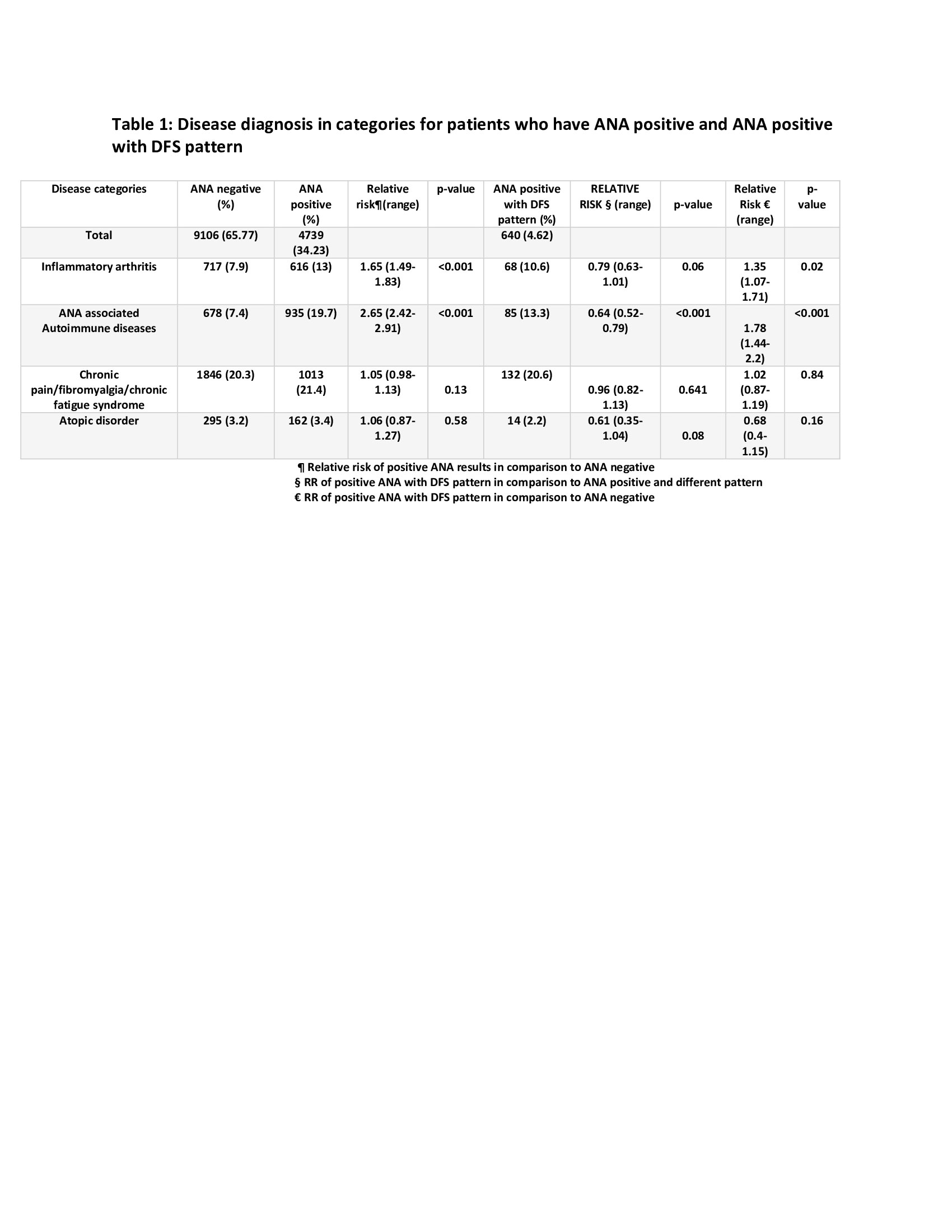
Background/Purpose: The clinical significance of Dense Fine Speckled (DFS) pattern Anti-nuclear antibodies (ANA) by indirect immunofluorescence method (IIF) is unclear and has been inversely associated with rheumatic disease. Our purpose was to determine associations between DFS pattern ANA and the disease categories of inflammatory arthritis, ANA associated rheumatic diseases (AARD), fibromyalgia/chronic pain syndrome/chronic fatigue syndrome and atopic disorder.
Methods: This retrospective study used data from patients tested for ANA by IIF between August 2017 to August 2019 at the University of Minnesota Medical Center. Comparisons between the diagnostic categories listed above were made for patients with negative ANA, positive ANA (any pattern) and DFS pattern. Individual disease diagnoses belonging to the above categories were also analyzed. The inflammatory arthritis category included Rheumatoid arthritis (RA), ankylosing spondylitis, and psoriatic arthritis. The disease category of AARD included systemic lupus erythematosus (SLE), systemic sclerosis (SSc), mixed connective tissue disease , idiopathic inflammatory myopathies, Sjogren’s syndrome (SS), and undifferentiated connective tissue disorder (UCTD). Atopic disorders included atopic dermatitis, allergic rhinitis, urticaria, and asthma. Frequency of Raynaud’s phenomenon (RP) was also calculated.
Results: 13,845 patients with an ANA during the study period were identified. 9106 (65.8%) had negative ANA and 4739 (34.2%) had positive ANA by IIF. 640 (4.6%) had ANA positive DFS patterns. Relative risk (RR) was calculated for diagnostic categories and individual diseases. For patients with positive ANA and DFS pattern, the RR for diagnostic codes of inflammatory arthritis categories [1.35 (1.07- 1.71), p=0.02] was higher when compared to the frequency of codes in ANA negative. RR for AARD among patients with DFS pattern was also higher [1.78 (1.44- 2.2), p < 0.001]. The frequency of AARD diagnostic codes was lower for patients with DFS pattern [0.64 (0.52- 0.79), p< 0.001] compared to ANA positive patients with all other patterns, consistent with published data. There was no significant difference of frequency of diagnostic codes for the rest of the disease categories when comparison was made between ANA positive DFS pattern and ANA positive with other patterns,
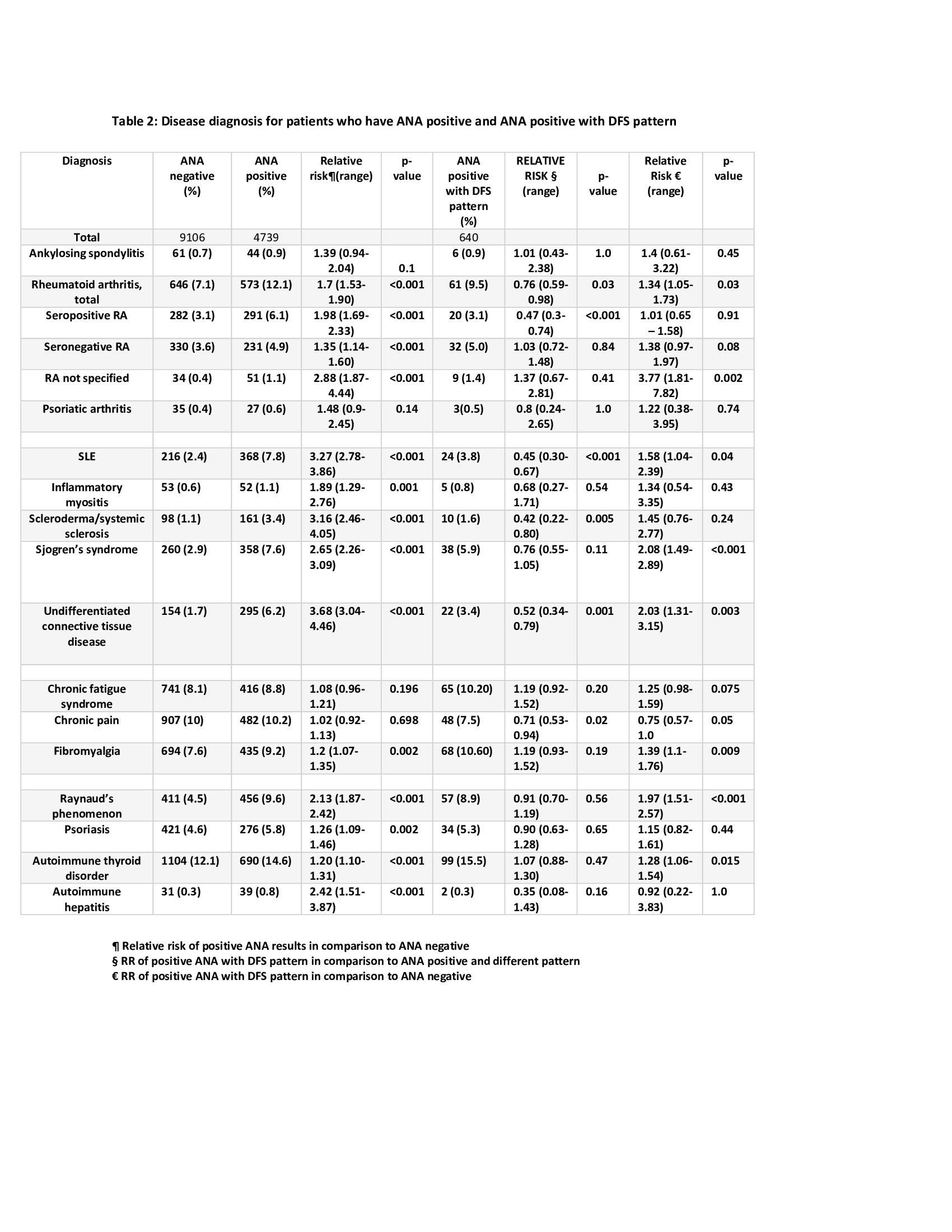
Individual disease diagnostic codes of RA were higher among DFS+ patients when compared to ANA patients. The frequency of diagnostic codes of SLE, SS, UCTD, fibromyalgia, RP, and autoimmune thyroid disease was also higher among patients with DFS pattern compared to ANA- patients. The frequency of diagnostic codes of seropositive RA was lower among patients with DFS pattern compared to ANA+ with all other patterns. The frequency of diagnostic codes of SLE, SSc, UCTD, and chronic pain was also lower among DFS+ patients, compared to those with ANA of all other patterns.
Conclusion: The frequency of diagnostic codes of RA, SS and Raynaud’s was higher among DFS pattern ANA compared to ANA negative group but was not significantly different from ANA positive with other patterns. This suggests that the presence of a DFS pattern should not be used to indiscriminately exclude the presence of a rheumatic disease.
To cite this abstract in AMA style:
Sapkota S, Molitor J, evans m, Kofoed B, Lord A, Robinson L, crosson J. Clinical Correlation of Dense Fine Speckled (DFS) Pattern of ANA [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/clinical-correlation-of-dense-fine-speckled-dfs-pattern-of-ana/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinical-correlation-of-dense-fine-speckled-dfs-pattern-of-ana/