Session Information
Session Type: Poster Session D
Session Time: 1:00PM-3:00PM
Background/Purpose: Cardiac sarcoidosis (CS) is potentially life-threatening and it typically causes heart failure, ventricular arrhythmia, AV block or sudden death. CS has been reported to account for 25% of sarcoidosis patient deaths, thus highlighting the importance of early diagnosis and treatment. Diagnostic challenges and lack of a unified screening approach make it difficult to estimate its prevalence. Immunosuppression is the mainstay of treatment, but there is paucity of data on optimal dose, duration and efficacy of steroids and synthetic (s) or biologic (b) disease-modifying anti-rheumatic drugs (DMARDs). The aim of this study is to describe the demographic and clinical characteristics of our CS patients, and to study their clinical response to steroids, synthetic and biologic DMARDs.
Methods: A retrospective cohort study with a prospective ongoing phase was conducted. ICD-10 codes were used to identify patients over 18 years old with sarcoidosis and CS followed at Montefiore Medical Center from 2017 to 2021. The following variables were recorded: demographics (age, sex, ethnicity), BMI, smoking status, presenting manifestations, histopathology (cardiac and extracardiac), imaging, treatment (corticosteroids and s/bDMARDs), dose and duration of therapy, steroid-sparing effect, response to treatment based on clinical and imaging improvement (echocardiogram, cardiac MRI, PET).
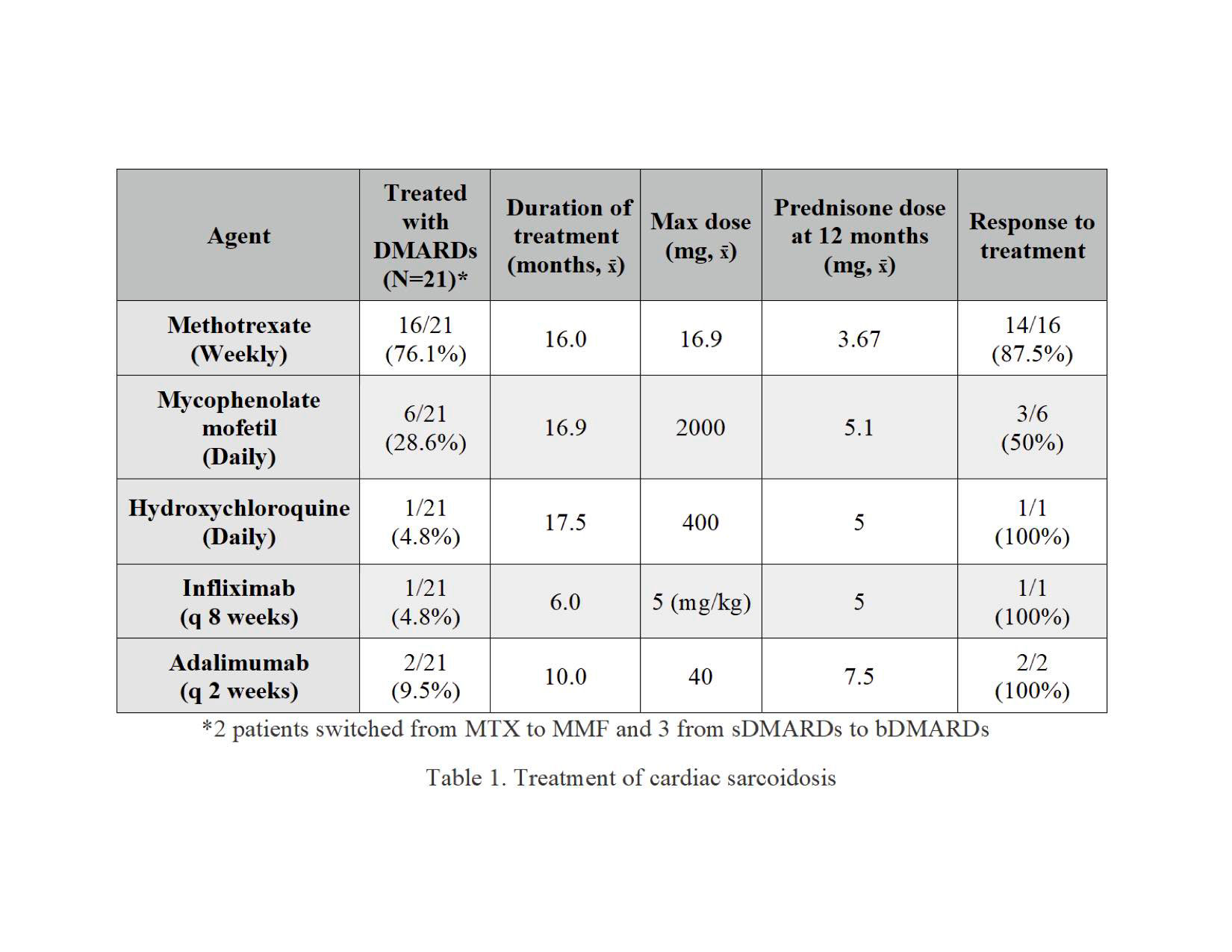
Results: 220 patients with sarcoidosis were identified. 154 (70%) female and 124 (56.4%) Black. 42 out of 220 (19.1%) met diagnostic criteria for CS (1,2). Mean age of CS patients was 61.6 years. 23 (54.8%) were male and 24 (57.1%) Black. Heart failure (54.8%), arrhythmias (47.6%) and heart block (28.6%) were the most common presenting manifestations. 28.6% had isolated CS. 5 (11.9%) underwent endomyocardial biopsy and 2 of them (40%) had histopathologic evidence of CS. Mean left ventricular ejection fraction (LVEF) was 40.6 % on echocardiogram, and 29 patients (69%) had PPM/ICD placed for arrhythmia prevention. 35 (83.3%) underwent cardiac MRI, 37 (88.1%) cardiac PET scan and 23 (62.3%) had a follow up PET. 33 (78.6%) CS patients were treated with corticosteroids for a mean duration of 17.3 months. 21 of them were also treated with sDMARDs and 3 were subsequently switched to bDMARDs (Table 1). Mean prednisone dose at 12 months was 4.8mg, and 11 patients (33%) were tapered off corticosteroids.
Conclusion: In our patient population, the prevalence of CS is 19.1%, which is higher than previously reported in the literature, suggesting CS may be underdiagnosed. There was a greater proportion of male patients in the CS population (54.8%) than the generalized sarcoidosis population (30%). This indicates that males with sarcoidosis may be more likely to have cardiac involvement. Patients treated with s/bDMARDs had a high response rate as reflected by clinical and imaging improvement. Steroid-sparing effect is suggested by the low prednisone dose at 12 months (Table1). Methotrexate was the most commonly used DMARD (76.2%). Randomized clinical trials are needed to establish robust guidelines for the treatment of CS.

To cite this abstract in AMA style:
Webster P, Rochlani Y, Loupasakis K. Cardiac Sarcoidosis: An Underdiagnosed, Life-threatening yet Treatable Disease [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/cardiac-sarcoidosis-an-underdiagnosed-life-threatening-yet-treatable-disease/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/cardiac-sarcoidosis-an-underdiagnosed-life-threatening-yet-treatable-disease/