Session Information
Date: Monday, November 18, 2024
Title: Abstracts: Systemic Sclerosis & Related Disorders – Clinical II
Session Type: Abstract Session
Session Time: 3:00PM-4:30PM
Background/Purpose: We have previously shown that fibroblast CD34 is low and alpha-smooth muscle actin (aSMA) is high in severe diffuse cutaneous systemic sclerosis (dcSSc) skin, and this pattern reverses with clinical improvement. The purpose of this study is to evaluate the relationship of skin fibroblast CD34 and aSMA expression and immune cell infiltration with disease duration, and to identify predictors of clinical improvement.
Methods: Baseline skin biopsies and clinical data were analyzed from 105 patients with dcSSc enrolled in the Lenabasum (N=79), Belimumab (N=18), or Nilotinib (N=8) clinical trials. CD34 and aSMA immunohistochemistry were scored semi-quantitatively (0-3): 0-1 = “low;” 2-3 = “high.” Immune cells (CD20+ B cells, CD3+ T cells, CD123+ plasmacytoid dendritic cells) were scored as cell count per 5 most populated high-powered fields (400X). Clinical and skin histological differences between those with early (< 18 months) versus later (≥ 18 months) disease duration (time since first non-Raynaud’s symptom) at trial enrollment and aSMA status were compared using Fisher’s exact, t-test, or Wilcoxon rank-sum.
Clinical improvement was defined as >5-point decrease in modified Rodnan skin score (mRSS) at 52 weeks. A multiple logistic regression model for improvement among 68 mycophenolate mofetil (MMF) users as a function of baseline predictors was developed. Model selection was by the (minimum) AIC criterion. Candidate predictors were CD34, aSMA, sex, baseline mRSS, CD20, CD3, CD123, belimumab use, disease duration at enrollment (< 18 or ≥18 months), and interactions of the predictors with disease duration.
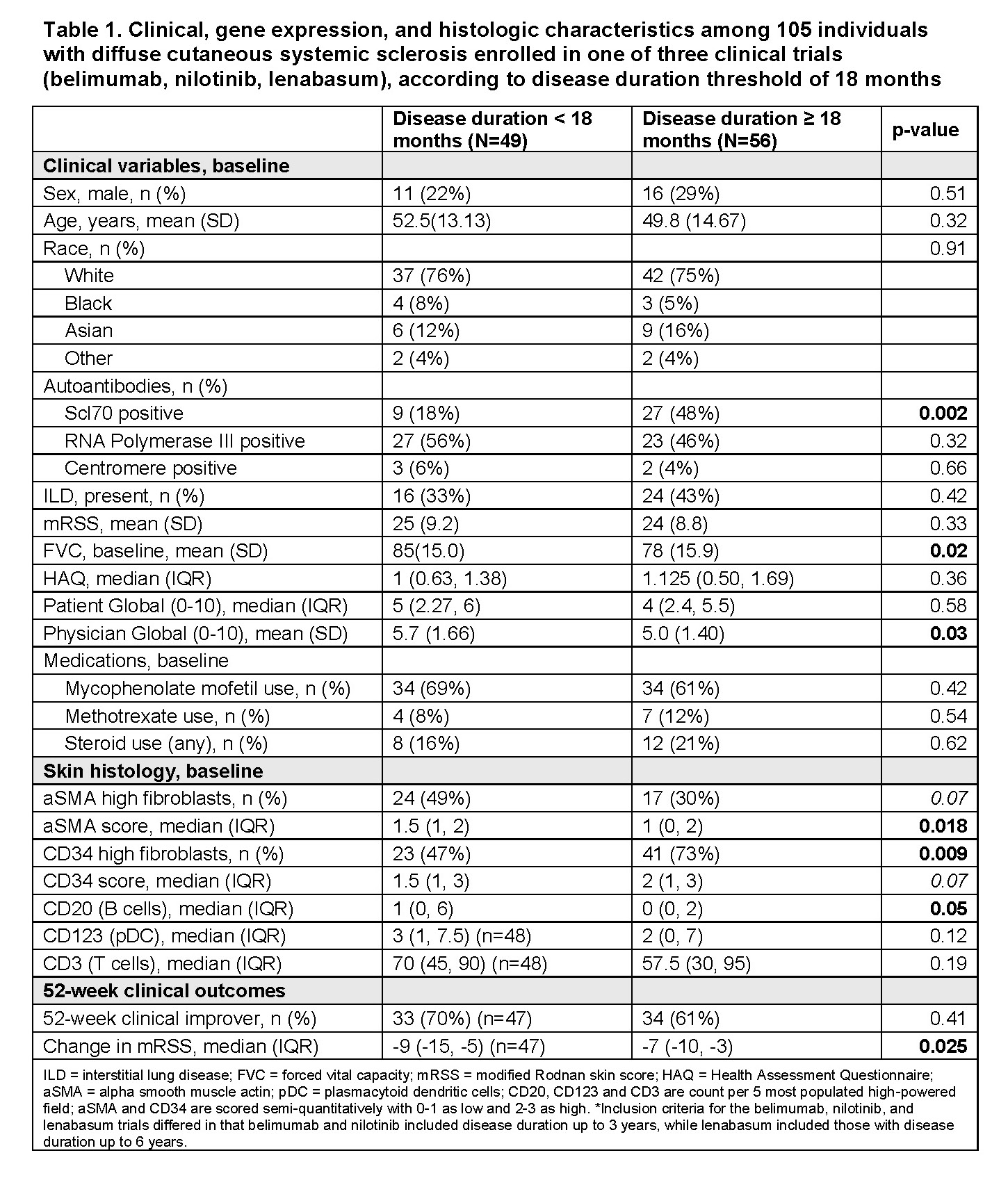
Results: Among 105 dcSSc trial participants, those with early (vs. later) SSc were more likely to have low CD34, high aSMA, and high median CD20+ B cell count. Despite these histology differences, there was no difference in baseline mRSS by disease duration (Table 1).
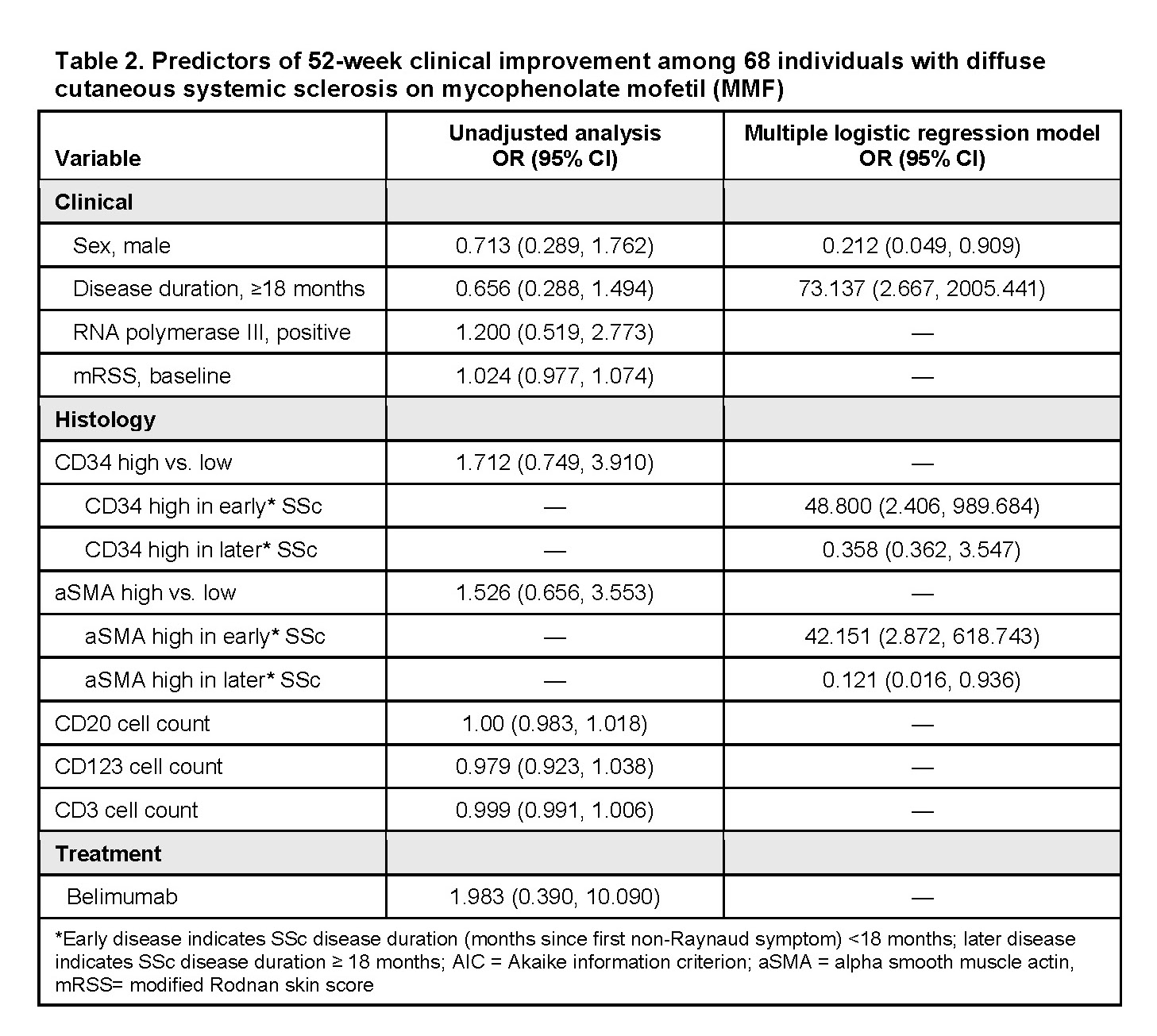
Median mRSS improvement was greater in those with early vs. later SSc in the full cohort and 68 patients treated with MMF (-9 vs. -7, p=0.025 and -11 vs. -7, p=0.038, respectively). In AIC-optimal multiple logistic regression for improvement on MMF, high CD34 and aSMA were associated with increased odds of improvement in early SSc, while high aSMA was associated with decreased odds of improvement in later SSc (Table 2). These results were similar in sensitivity analyses that included baseline mRSS, RNA polymerase III, CD20, CD3, CD123, and belimumab use.
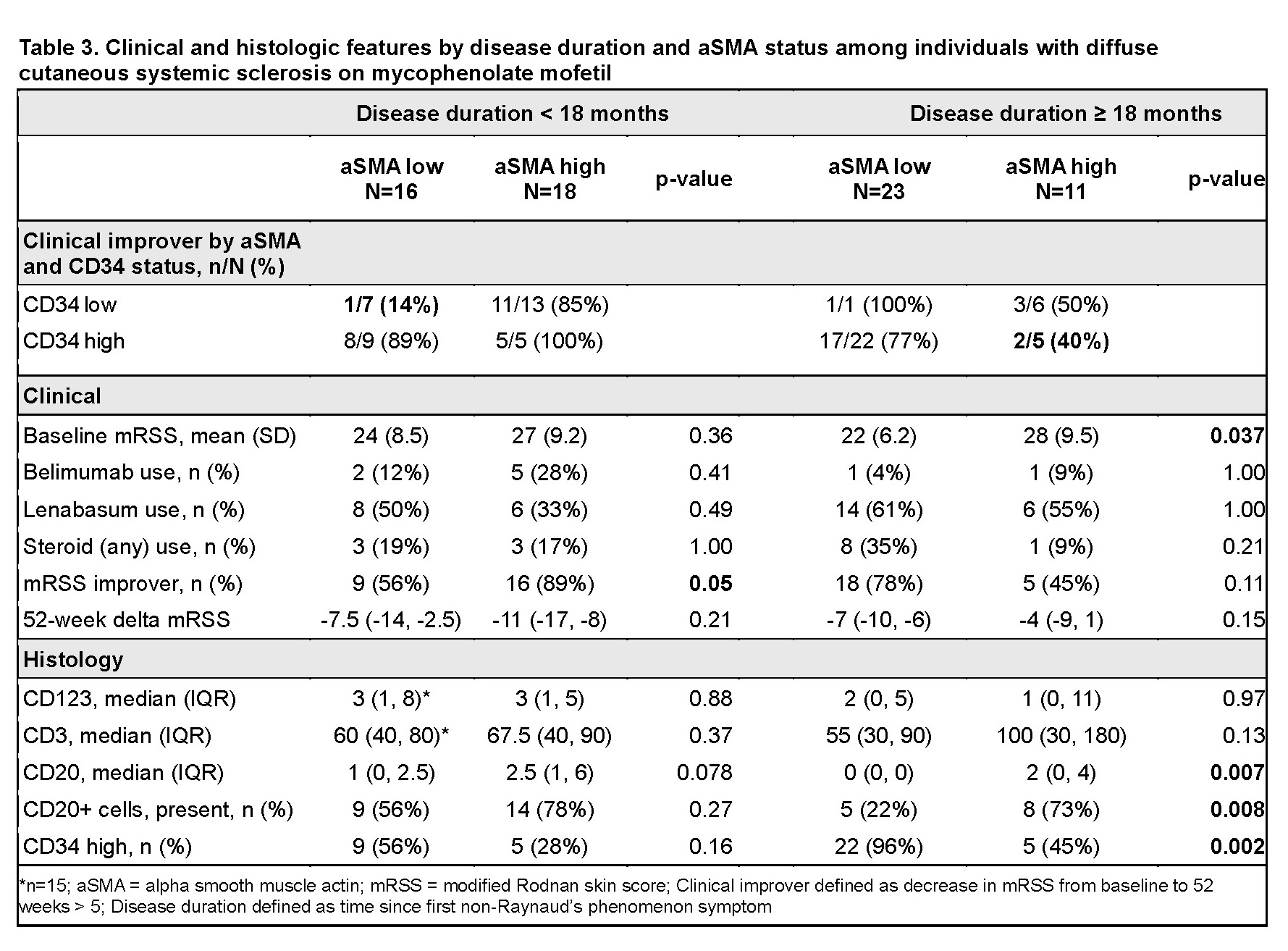
Given that high aSMA predicts improved outcomes early and worse outcomes in later SSc, we sought to better understand the role of sustained aSMA elevation in later disease. While no differences were seen in immune infiltrates by aSMA groups in early SSc, in later SSc, B cells were more often present in aSMA high vs. low skin (73% vs. 22%, p=0.008) (Table 3).
Conclusion: Early vs. later SSc at trial enrollment was associated with lower CD34, higher aSMA, and increased B cells, despite similar baseline mRSS. In early SSc, high CD34 and aSMA are associated with increased likelihood of improvement on MMF. However, in later SSc, persistently elevated aSMA was associated with decreased likelihood of improvement and increased B cells. Those with later SSc and high aSMA may benefit from additional treatment beyond MMF.
To cite this abstract in AMA style:
Lakin K, Spiera R, Spivack J, Zhang Y, Gordon J, Orange d. Baseline Fibroblast Immunophenotype Predicts Clinical Improvement Among Individuals with Early Diffuse Cutaneous Systemic Sclerosis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/baseline-fibroblast-immunophenotype-predicts-clinical-improvement-among-individuals-with-early-diffuse-cutaneous-systemic-sclerosis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/baseline-fibroblast-immunophenotype-predicts-clinical-improvement-among-individuals-with-early-diffuse-cutaneous-systemic-sclerosis/