Session Information
Session Type: Poster Session D
Session Time: 1:00PM-3:00PM
Background/Purpose: Juvenile Dermatomyositis(JDM) is heterogenous disease with many presentations. The underlying immune pathophysiology of JDM remains complex with varying phenotypes. B Cells remain a critical element in the pathophysiology both through the production of pathogenic antibodies but also as a target for the treatment of JDM. In order to better understand the role of B Cells in JDM we explored the associations of elevated B Cells in patients with JDM.
Methods: We queried the Cure JM Biorepository and Registry which houses patient samples of patients with a diagnosis of JDM or overlap myositis. A total 135 patients with untreated JDM/Overlap myositis were identified. The patients were divided into two groups based on age adjusted B cell percentage with 88 patients in the normal B cell percentage group and 42 in high B cell percentage group. The 5 patients with low B cells for age were excluded. We obtained the age, sex, ethnicity, duration of untreated disease, disease activity score, CMAS, neopterin, ESR, myositis specific antigen (MSA), and capillary end row loops room from the registry for the included patients. We also measured B Cell values prior to treatment, after 1-3 months of treatment and after weaning steroids.
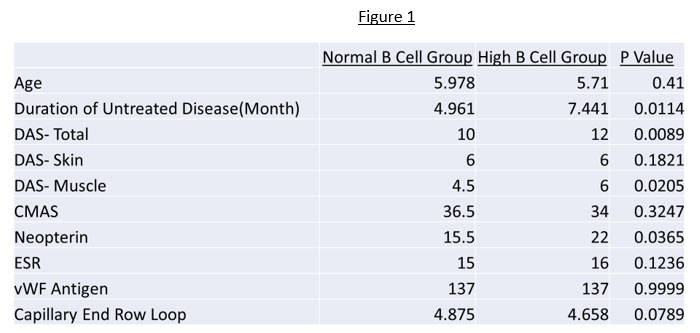
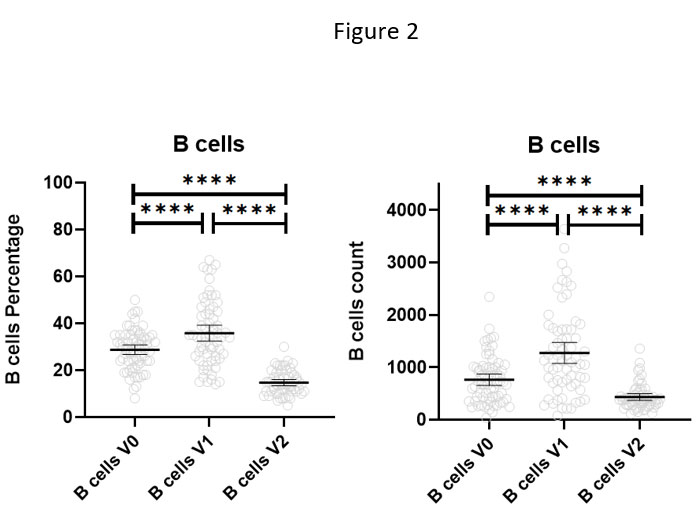
Results: Mann Whitney testing was used to compare the above parameters between the high and normal B cell groups. Duration of untreated disease, DAS total, DAS-Muscle, and neopterin were higher in the high B cell group and statistically significant as in Figure 1. There were no statistically significant differences in Age, DAS-Skin, ESR, vWF antigen, or nailfold capillary end loops. Patient B cell percentage and number was significantly higher after 1-3 months of therapy and then significantly lower on completion of therapy as shown in Figure 2.
Conclusion: This study shows that JDM patients with high B cells have higher neopterin, DAS and DAS-muscle than the normal B cell group. The association of high B cells with these markers of JDM disease activity supports the role of using B cell count as a marker of B cell activity. Curiously B cells both in absolute number and percentage appear to persist during early treatment but later decrease on completion of steroids. This may speak to initial B cell steroid resistance or B cell dysregulation which may have a role in the prolonged steroid need in some patients.
To cite this abstract in AMA style:
Costin C, Morgan G, Khojah A, Pachman L. B Cell Count in Juvenile Dermatomyositis: A Biomarker of Disease [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/b-cell-count-in-juvenile-dermatomyositis-a-biomarker-of-disease/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/b-cell-count-in-juvenile-dermatomyositis-a-biomarker-of-disease/