Session Information
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Feared complications of systemic sclerosis (SSc) affect the pulmonary system, with pulmonary hypertension and interstitial lung disease being common causes of mortality. Baseline and annual transthoracic echocardiography (TTE) screening for pulmonary hypertension in asymptomatic patients is recommended by experts from the American College of Cardiology, American Heart Association, European Society of Cardiology, and European Respiratory Society.1 For screening of interstitial lung disease (ILD) in SSc, it is recommended that computed tomography (CT) of the chest in addition to pulmonary function tests (PFTs) be obtained at baseline. Based on expert opinion, PFTs should then be obtained every two years in asymptomatic patients with normal diffusing capacity.2
The aim of our quality improvement study was to assess the compliance rate of the Division of Rheumatology at Loyola University Medical Center in screening patients for SSc-related lung disease within one year of diagnosis, or at the initial encounter in those patients with a preexisting diagnosis of SSc.
Methods: Patients with a diagnosis of SSc at Loyola University Medical Center between January 1, 2010 and June 1, 2019 were screened for study inclusion. Medical records were retrospectively reviewed and data collected included demographic information and dates of PFTs, TTEs, and chest CT scans. The primary endpoint was the proportion of patients who have all three lung disease screening tests done within one year of diagnosis or at the initial encounter in patients with a preexisting diagnosis of SSc. Secondary endpoints included the proportion of patients having at least one screening test done within this same time frame, as well as the frequency of follow-up PFTs and TTEs. Nonparametric univariate statistics were used to quantify the frequency in which SSc patients had PFTs and TTEs performed.
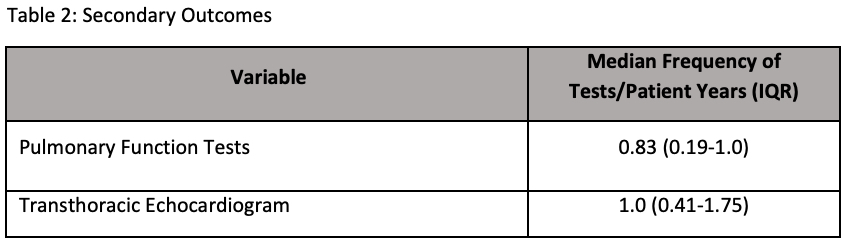
Results: A total of 122 patients were screened, and 65 fulfilled inclusion criteria. The primary outcome was reached in 29 patients (44.62%), and not reached in 36 patients (55.38%). At least one lung disease screening test was performed within one year of diagnosis or initial visit in 60 patients (92.31%), and not performed in 5 patients (7.69%). Of the three lung disease screening tests CT of the chest was obtained the most infrequently, with 35 patients (53.85%) having the test performed, and 30 patients (46.15%) not having the test performed. The median number of PFTs per patient years was 0.83 (IQR 0.19-1.0), while the median number of TTEs per patient years was 1.0 (IQR 0.41-1.75).
Conclusion: Our study showed that while the majority of SSc patients have at least one lung disease screening test within one year of diagnosis or initial visit, only about half of the patients had CT of the chest performed. Several cohorts involving SSc patients have suggested that more than half of patients may have ILD at diagnosis despite an absence of symptoms. Therefore, efforts should be made to obtain CT scans as early as possible in the course of diagnosis, and further quality improvement measures should be instituted to help achieve this goal.
- Galie N, et al. Eur Respir J2015; 46: 903–975.
- Kane GC, et al. Respir Med 1996; 90:223.


To cite this abstract in AMA style:
Herrmann M, Aouhab Z. Assessing Adherence to Screening of Systemic Sclerosis-Related Lung Disease [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/assessing-adherence-to-screening-of-systemic-sclerosis-related-lung-disease/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/assessing-adherence-to-screening-of-systemic-sclerosis-related-lung-disease/