Session Information
Date: Saturday, November 16, 2024
Title: Imaging of Rheumatic Diseases Poster I: Inflammatory Arthritis
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Patients with RA are at increased risk of cardiovascular disease (CVD) compared to the general population. In a prior study of RA patients with overall low estimated atherosclerotic cardiovascular risk (ASCVD), nearly 50% had evidence of coronary microvascular dysfunction (CMD) and 23% had a detectable high sensitivity cardiac troponin (hs-cTnT). We hypothesized that CMD, as measured by coronary flow reserve (CFR) and detectable troponin can serve as markers of a subclinical early inflammatory cardiac phenotype associated with increased future CV risk. The objective of this study was to determine the association of these findings among RA subjects with no CAD with future atherosclerotic plaque burden in RA.
Methods: RA subjects were selected from the completed LiiRA study (NCT02714881); all subjects underwent a stress myocardial perfusion PET (cardiac PET) and measurements for hs-cTnT. Coronary flow reserve (CFR) was calculated from cardiac PET data to determine the presence of CMD (CFR< 2.5). All LiiRA subjects with an abnormal stress test (evidence of CAD) were excluded from the present study. From this group, we recruited subjects who fulfilled the inclusion criteria for a case: CFR< 2.5 and/or detectable hs-cTnT, or control: CFR >2.5 and no detectable hs-cTnT. All subjects underwent a computed coronary tomography angiography (CCTA) (must be ≥2 years since the baseline LiiRA cardiac PET). Advanced plaque quantification was performed with AutoPlaque software, including the non-calcified plaque (NCP) volume, calcified plaque (CP) volume, and the pericoronary fat attenuation index (PCAT). The baseline estimated 10-year ASCVD risk was calculated for all study subjects. Differences in coronary plaque characteristics were compared between cases and controls using t-tests or Wilcoxon rank sum. Correlations between the baseline CFR and future CCTA was determined using Spearman’s.
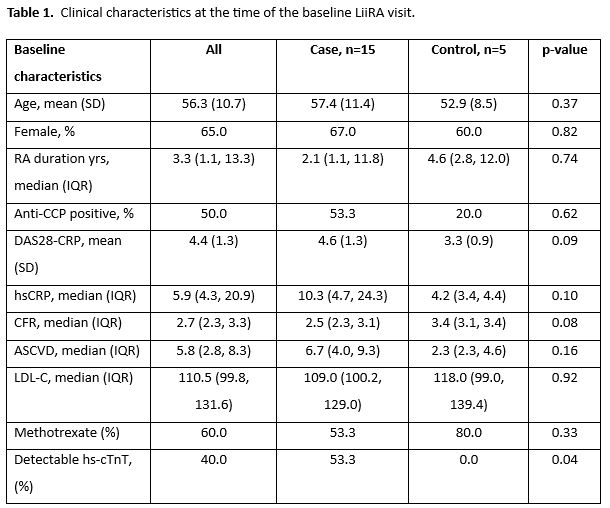
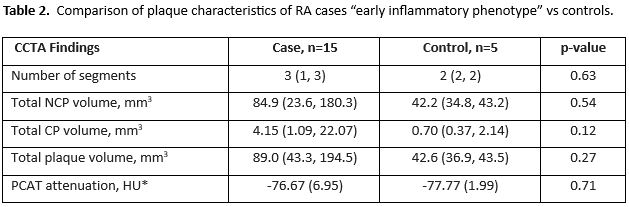
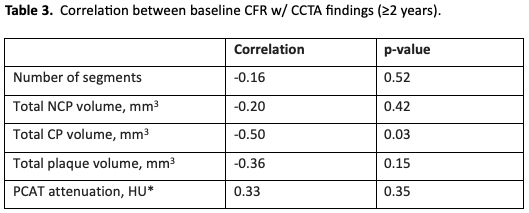
Results: We recruited n=20 subjects, n=15 with the “early inflammatory cardiac phenotype” and n=5 controls. There was no significant difference in the baseline demographics and estimated ASCVD risk; the median 10-year estimated ASCVD risk in this population was 5.8% (borderline) (Table 1). No significant difference was observed in the CCTA plaque characteristics between cases and controls, including NCP, CP, and PCAT (Table 2). For the overall cohort, a lower CFR at baseline (evidence of CMD) was correlated with higher CP volume at 2 years (Table 3).
Conclusion: Early findings of CMD or detectable troponin was associated with higher future atherosclerotic plaque burden at ≥2 years. These findings suggest that both mild coronary vasomotor dysfunction or the presence of detectable troponin can inform earlier primary prevention therapies among RA patients at low/borderline ASCVD risk by traditional risk factors.
*among n=8 cases and n=2 controls
*among n=8 cases and n=2 controls
To cite this abstract in AMA style:
Weber B, Liu F, Jeffway M, Weisenfeld D, McDermott G, Massarotti E, Coblyn J, Weinblatt M, Di Carli M, Dey D, Liao K. An Early Inflammatory Cardiac Phenotype and Association with Future Coronary Plaque Burden in Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/an-early-inflammatory-cardiac-phenotype-and-association-with-future-coronary-plaque-burden-in-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/an-early-inflammatory-cardiac-phenotype-and-association-with-future-coronary-plaque-burden-in-rheumatoid-arthritis/