Session Information
Session Type: Poster Session C
Session Time: 1:00PM-3:00PM
Background/Purpose: Rheumatoid arthritis (RA) predisposes patients to heart failure (HF), a leading cause of hospitalization in the US. While improvements in all-cause and cardiovascular (CVD) mortality have been observed in contemporary RA cohorts, it is unclear whether similar improvements have occurred for HF-related outcomes. And though HF risk in RA is reported independent of ischemic CVD, study of the relative incidence of HF with reduced ejection fraction (HFrEF) on a population level is limited. Thus, we examined temporal trends in the risk of incident HF in RA and explored the burden of HFrEF in RA vs non-RA patients.
Methods: We conducted a retrospective, matched cohort study in the Veterans Health Administration (VA) from 1/2000 through 12/2019. Incident RA patients (≥2 ICD codes for RA, rheumatologist diagnosis, and positive autoantibody or DMARD fill) were matched up to 1:10 on age, sex, and enrollment year to patients without RA diagnosis codes. Incident HF was identified by a primary hospital discharge diagnosis or HF-related death, linking National VA data with Medicare and the National Death Index. Echocardiogram-derived LVEF was extracted from clinical notes through a previously validated natural language processing tool. Matched pairs with no history of HF were followed to incident HF, death, or end of study period, censoring patients who did not receive VA care for ≥365 days. Multivariable Cox regression, clustered by matched pairs, was used to examine the association of RA with incident HF and HF-related death adjusting for demographics, smoking status, body mass index, and comorbidity burden. To examine temporal trends in HF risk, analyses were stratified by RA diagnosis year (2000-05, 2006-11, 2012-17). We then explored the relative burden of HFrEF (LVEF ≤40%), using the most proximate LVEF prior to a HF event or < 30 days following a discharge date if prior LVEF was missing.
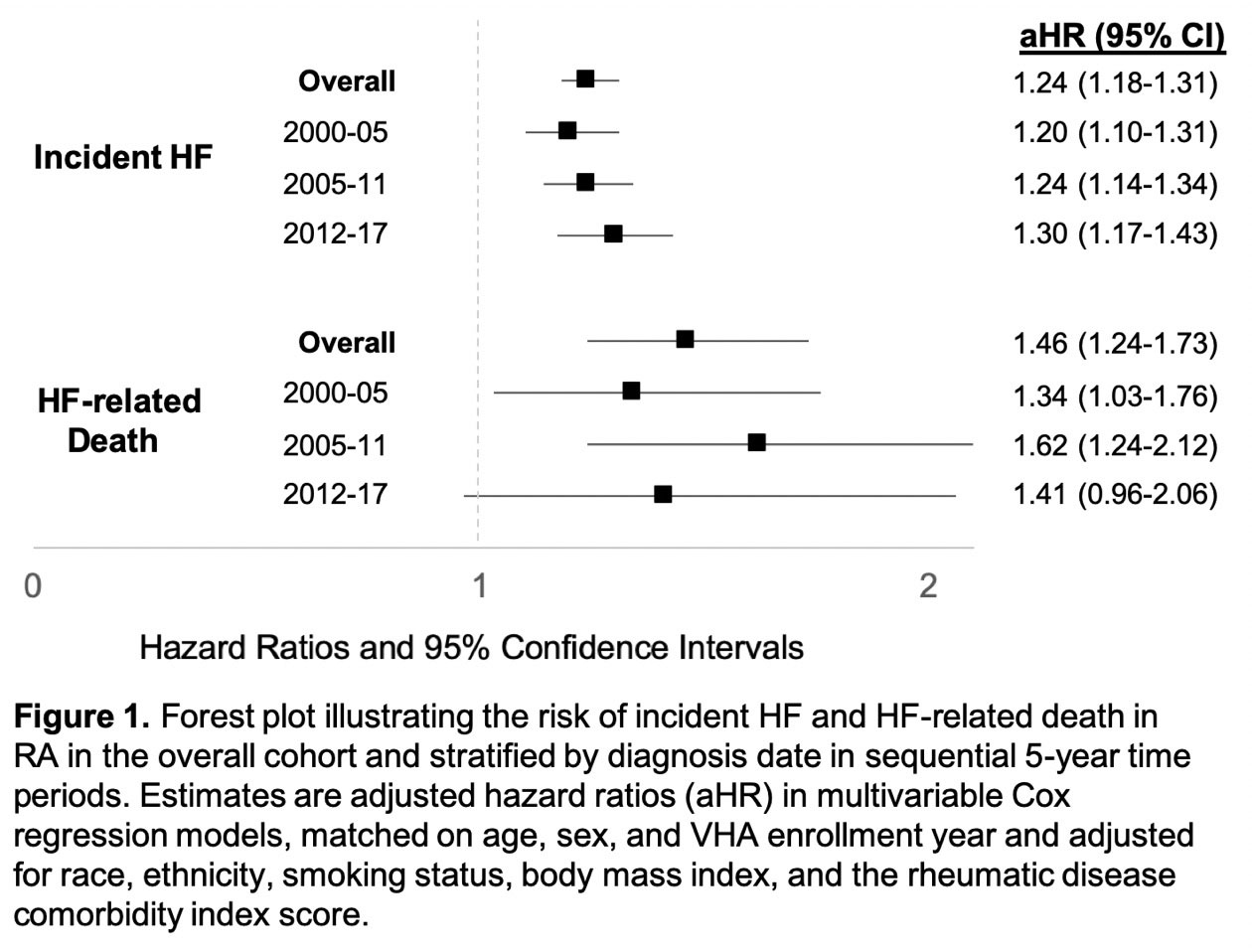
Results: We matched 29,451 incident RA patients to 229,028 patients without RA. RA patients had a mean age of 63 years and were predominantly male (85.9%). Over 1,391,380 person-years (PY; mean follow-up 5.4 years), we observed 1,849 incident HF events in RA (10.7 per 1000 PY) vs. 8,797 events in non-RA (7.2 per 1000 PY). Amongst those with available LVEF data ( >70% of patients), the majority of RA and non-RA patients who developed HF had an LVEF >40% (73.2% in RA vs 71.0% in non-RA, p=0.09). After multivariable adjustment, RA patients were at increased risk of HF (adjusted hazard ratio [aHR] 1.24, 95% CI 1.18-1.31) and HF-related death (aHR 1.46, 95% CI 1.24-1.73) (Figure 1). No temporal improvements in risk of HF (range aHR 1.20-1.30) or HF-related death (aHR 1.34-1.62) were observed.
Conclusion: In this large, matched cohort study, we observed a 24% increased risk of incident HF and 46% increased risk of HF-related death in patients with RA, primarily related to HF with LVEF >40%. Contrasting previously reported improvements in all-cause and CVD-related mortality, no improvements in RA-related HF risk were observed over two decades of observation. These findings highlight the need to elucidate RA-related mechanisms underpinning this risk and develop effective HF management strategies to improve longevity in RA.
To cite this abstract in AMA style:
Johnson T, Yang Y, Roul P, Alonso W, Baker J, Sauer B, Cannon G, Mikuls T, England B. An Increased Risk of Heart Failure and Heart Failure-Related Death Persists in Rheumatoid Arthritis: A National, Matched Cohort Study from 2000 to 2019 [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/an-increased-risk-of-heart-failure-and-heart-failure-related-death-persists-in-rheumatoid-arthritis-a-national-matched-cohort-study-from-2000-to-2019/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/an-increased-risk-of-heart-failure-and-heart-failure-related-death-persists-in-rheumatoid-arthritis-a-national-matched-cohort-study-from-2000-to-2019/