Session Information
Date: Monday, November 8, 2021
Session Type: Poster Session C
Session Time: 8:30AM-10:30AM
Background/Purpose: RA is a complex multisystem disease, which, untreated, results in debilitating joint damage, excess morbidity, and premature mortality. Previous research has demonstrated an association between early treatment and improved outcomes; however, there is often a delay between symptom onset and diagnosis. We investigated the demographic and clinical features associated with delay in RA diagnosis and the impact of delayed diagnosis on disease activity in U.S. Veterans.
Methods: We studied patients in the Veterans Affairs Rheumatoid Arthritis (VARA) registry which prospectively captures RA disease activity and severity measures from 12 VA Medical Centers. We included patients who reported a date of symptom onset within 5 years of RA diagnosis to avoid bias related to inaccurate recall. Patient demographics, date of symptom onset and diagnosis (collected by self-report at the time of enrollment); and the results of RF, Anti-CCP, CRP, and tender and swollen joint counts were extracted from the registry. Disease activity measures at enrollment, and 2-years after diagnosis, for RAPID3, CDAI, DAS28ESR and DAS28CRP were calculated. Early diagnosis was defined as diagnosis within 6 months of symptom onset. The relationship between pre-hypothesized study variables and the time to diagnosis was evaluated using contingency analysis and Kruskal-Wallis or Wilcoxon tests for non-normative data. Two-year post-diagnosis disease activity scores were averaged to estimate influence of a delay in diagnosis on subsequent disease control.
Results: At the time of the study there were 2,996 patients eligible for the study and 1,454 were included. The primary reasons for exclusion were patients unable to recall symptom onset date (1,169) and diagnosis date that was greater than 5 years after onset date (373). Of those included, 485 veterans were diagnosed within 6 months and 969 were diagnosed between 6 months and 5 years. Delayed diagnosis was associated with younger age, 53.7 years vs 56.2 years. (Table 1) Those with delayed diagnosis also had higher rates of current smoking. There were no significant differences in terms of family history of RA, education level, or race. No difference was noted in enrollment TJC, SJC, CRP, disease activity scores or rates of RF or CCP positivity. TJC and SJC also did not differ between groups at 2 years, however, there were lower median RAPID3 and CDAI scores in the early diagnosis group, as well as a larger change from baseline scores. No statistical difference was noted in the DAS28CRP scores at 2 years while the DAS28ESR slightly favored the early group.
Conclusion: In this veteran cohort, where the model of access to care is substantially different from typical U.S. healthcare systems, traditional predictors of delay in RA diagnosis (older age, race, and education level) were not noted to contribute. While 2-year post diagnosis TJC and SJC were not different between the groups, differences in RAPID3 and CDAI suggest that earlier diagnosis may result in better long-term patient-reported outcomes. Additional research is needed to understand why younger age and smoking might lead to delayed diagnosis.
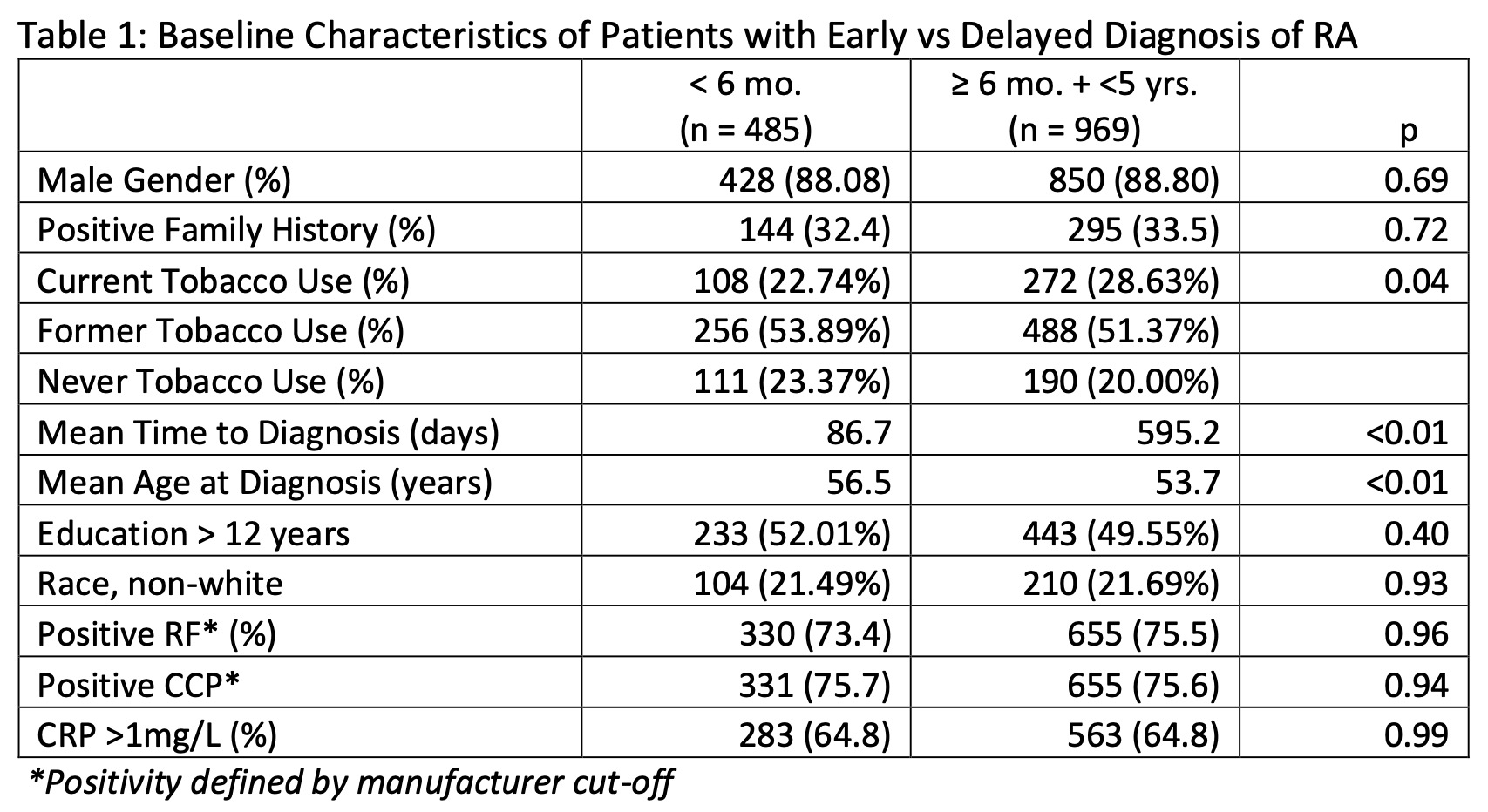 Table 1: Baseline Characteristics of Patients with Early vs Delayed Diagnosis of RA
Table 1: Baseline Characteristics of Patients with Early vs Delayed Diagnosis of RA
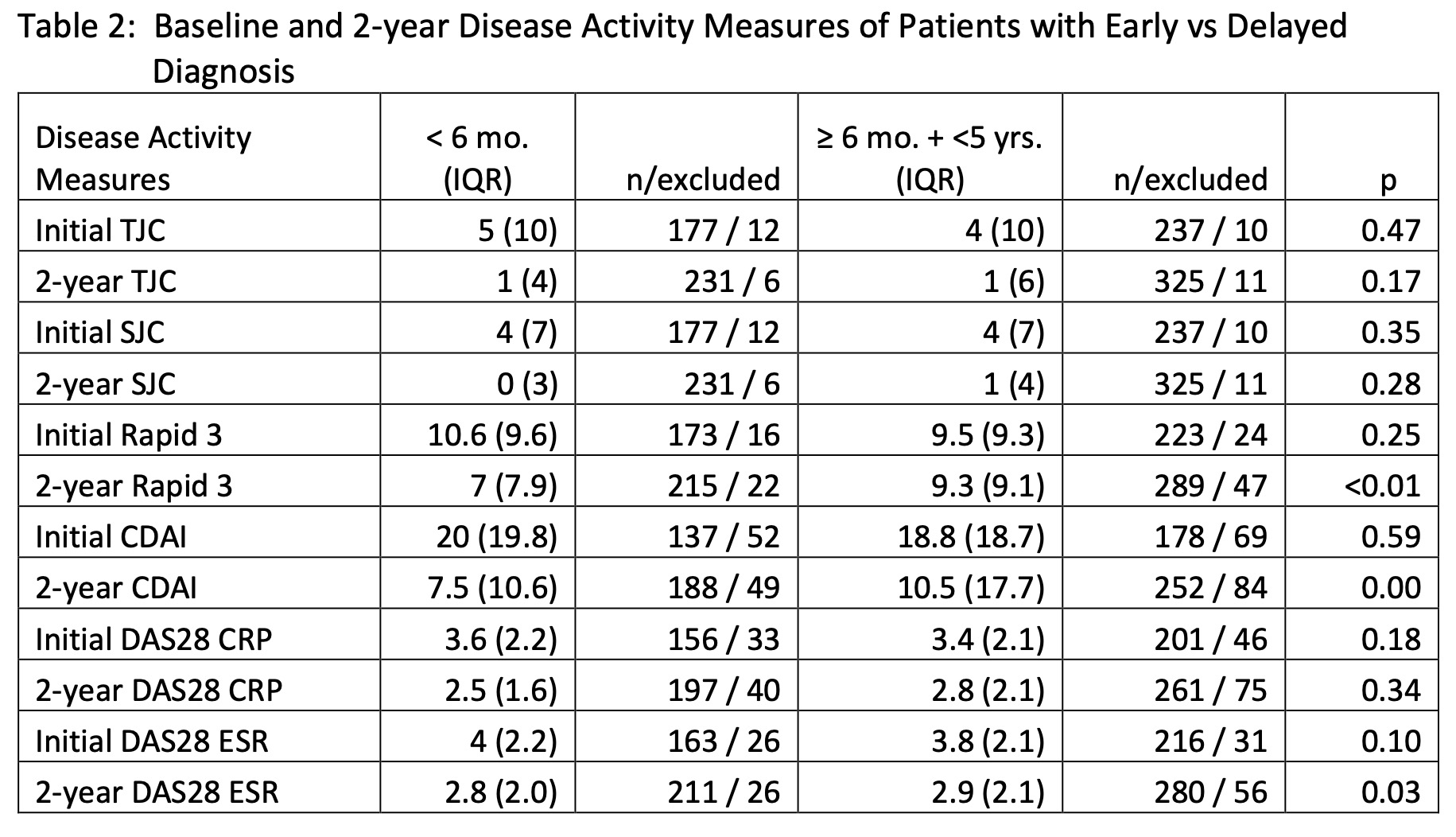 Table 2: Baseline and 2-year Disease Activity Measures of Patients with Early vs Delayed Diagnosis
Table 2: Baseline and 2-year Disease Activity Measures of Patients with Early vs Delayed Diagnosis
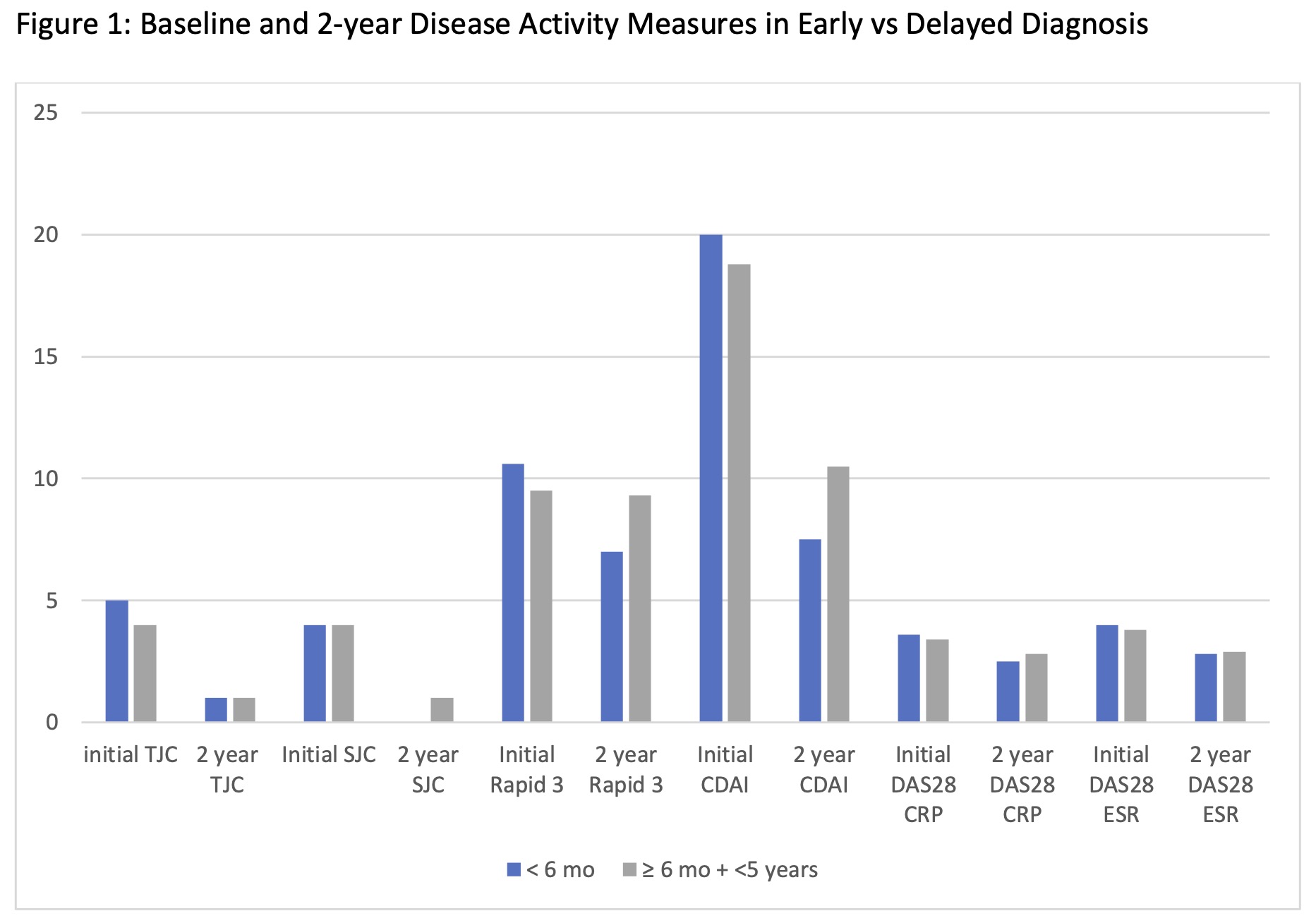 Figure 1: Baseline and 2-year Disease Activity Measures in Early vs Delayed Diagnosis
Figure 1: Baseline and 2-year Disease Activity Measures in Early vs Delayed Diagnosis
To cite this abstract in AMA style:
Taylor S, England B, Baker J, Sauer B, Richards J. Younger Age and Smoking Status Are Associated with Delayed Diagnosis of Rheumatoid Arthritis in a U.S. Veteran Population [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/younger-age-and-smoking-status-are-associated-with-delayed-diagnosis-of-rheumatoid-arthritis-in-a-u-s-veteran-population/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/younger-age-and-smoking-status-are-associated-with-delayed-diagnosis-of-rheumatoid-arthritis-in-a-u-s-veteran-population/