Session Information
Session Type: Abstract Session
Session Time: 2:00PM-3:30PM
Background/Purpose: Knee osteoarthritis (OA) is a leading cause of functional limitation (FL) in older adults, with difficulty climbing stairs often the first-reported limitation. Overall increased difficulty with stair climbing is associated with greater risk of developing FL and receiving a knee replacement (KR). However, little is known about the relation of the direction of stair climbing difficulty (ascending or descending) with the development of knee OA-related outcomes. Therefore, the purpose of this study was to examine the relationship of difficulty ascending and descending the stairs with incident FL and KR in adults with or at high risk for knee OA.
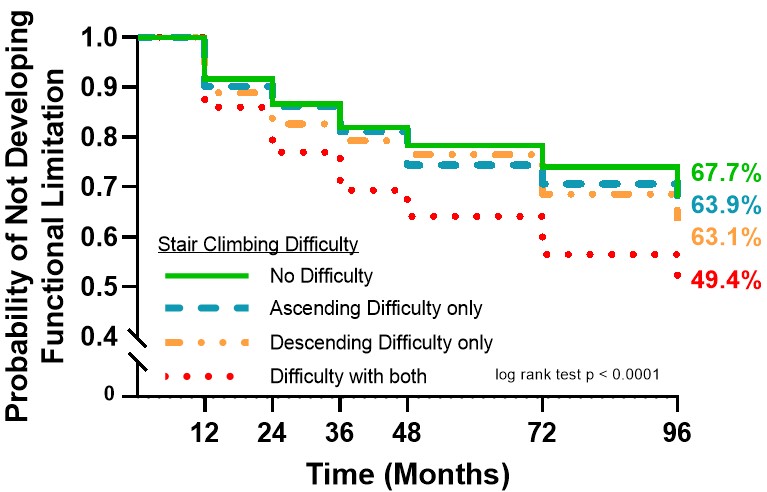
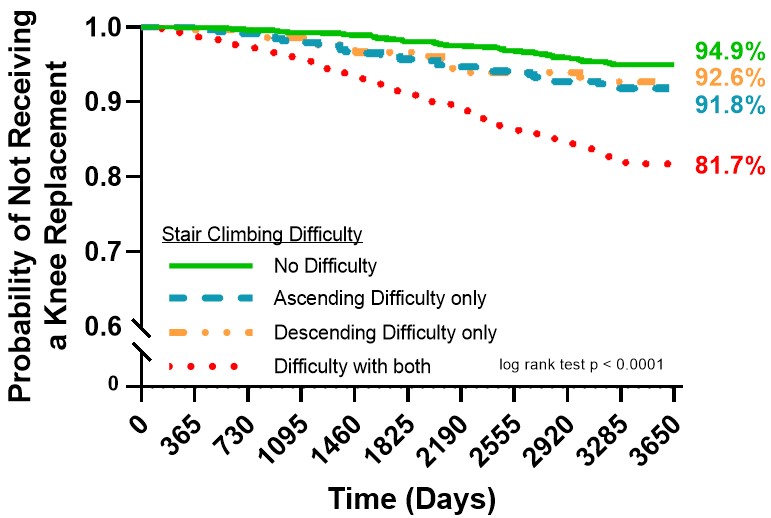
Methods: We used data from the Osteoarthritis Initiative (OAI). Stair climbing difficulty was assessed at baseline (BL) using two questions from the WOMAC: 1.) What degree of difficulty do you have with ascending stairs? and 2.) What degree of difficulty do you have with descending stairs? Choices included: none, mild, moderate, severe, extreme. A 4-level exposure combining difficulty with ascending and descending stairs was created: no difficulty with either, difficulty with ascending only, difficulty with descending only, difficulty with both ascending and descending. FL was defined as walking speed < 1.22 m/s over 20 meters and was collected at BL, 12-, 24-, 36-, 48-, 72-, and 96-month follow-up. 1.22 m/s has been previously used to represent poor function. KR was defined as any type of KR and was collected from the BL visit until 10 years later. Separate analytic samples were used for each outcome and only included those without the outcomes at BL. We produced Kaplan-Meier survival curves for cumulative incidence of FL and KR and used Cox proportional hazards regression to calculate hazard ratios (HR) and 95% confidence intervals (CI), adjusted for age, sex, BMI, race, radiographic knee OA, VAS pain, and presence of comorbidity.
Results: 2866 participants (mean age = 60.3 years old, 53.8% female, mean BMI = 28.1 kg/m2) were included in the FL sample and 4523 participants (mean age = 61.3 years old, 58.3% female, BMI = 28.7 kg/m2) were included in the KR sample. 957 participants developed FL (Figure 1) and 438 participants received a KR (Figure 2) during follow-up. Compared to those without any difficulty ascending and descending stairs, those with difficulty in both ascending and descending stairs were at a 44% greater hazard of FL and a 132% greater hazard of KR, those with only difficulty ascending but not descending stairs were at a 7% greater hazard of FL and a 64% greater hazard of KR, and those with only difficulty descending but not ascending stairs were at a 10% greater hazard of FL and a 40% greater hazard of KR (Table 1).
Conclusion: Adults with knee OA who have any amount of difficulty with both ascending and descending stairs are at greater risk of developing both walking speed FL and receiving a KR compared to those with no difficulty. Self-reported stair climbing difficulty may be useful as a functional vital sign for identifying those at early risk for FL and KR and in need of further evaluation and treatment.

To cite this abstract in AMA style:
Jakiela J, Bye T, Liles S, White D. Up or Down: Does Direction of Stair Climbing Difficulty Matter for Incident Functional Limitation and Knee Replacement in Knee Osteoarthritis? [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/up-or-down-does-direction-of-stair-climbing-difficulty-matter-for-incident-functional-limitation-and-knee-replacement-in-knee-osteoarthritis/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/up-or-down-does-direction-of-stair-climbing-difficulty-matter-for-incident-functional-limitation-and-knee-replacement-in-knee-osteoarthritis/