Session Information
Date: Monday, October 27, 2025
Title: (1306–1346) Rheumatoid Arthritis – Diagnosis, Manifestations, and Outcomes Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Venous thromboembolism (VTE) is more common in patients with rheumatoid arthritis (RA) and can present as deep vein thrombosis (DVT) or pulmonary embolism (PE). The changing risks of VTE in patients with RA over time and in relation to RA disease characteristics and treatments have not been comprehensively studied in longitudinal population-based cohorts. We aimed to estimate the risk of incident VTE (PE and DVT) in patients with RA vs the general population, to identify risk factors for VTE, mortality after VTE and time trends of VTE in RA.
Methods: This retrospective population-based cohort study included residents of a geographically defined area, meeting the 1987 ACR RA criteria in 1980-2019 and comparators from the same population with similar demographics. DVT/PE were identified by >2 ICD 9/10 codes >30 days apart and confirmed by manual record review. Cox proportional hazards models were used to compare incident VTE in RA vs. non-RA cohort, adjusting for demographics, smoking and obesity. Cumulative incidence of DVT, PE and total VTE was estimated, adjusting for competing risk of death. Cox models were used to examine risk factors for VTE in RA and to compare mortality in RA vs non-RA.
Results: 2818 individuals were included: 1409 with RA (62% RF/CCP-positive) and 1409 without RA, mean age 55.9 years, 68% women in both groups. Mean follow-up: 14.0 and 14.9 years in the RA and non-RA cohort respectively. DVT developed in 105 and 52 people with and without RA respectively. PE developed in 84 and 55 people with and without RA respectively. Persons with RA had a significantly increased risk of incident DVT (HR 2.26, 95%CI 1.62-3.17) and PE (HR 1.61, 95%CI 1.14-2.27). There was a significant difference in RA as a risk factor for VTE in two of the decades: 1980-1989 (HR 1.57; 95%CI 0.86-2.89), 1990-1999 (HR 2.68, 95%CI 1.55-4.63), 2000-2009 (HR1.80, 95%CI 1.13-2.86), 2010-2019 (HR 1.74, 95%CI 0.95-3.17). There was a significant increase in PE risk in both persons with RA onset after 2000s vs before 2000s (HR 2.00, 95%CI 1.21-3.32) and in the non-RA cohort (HR 2.70, 95%CI 1.38-5.28). Adjusted for age, sex, and calendar year, risk factors for DVT in RA included age, BMI >30 kg/m2, Charlson comorbidity index, rheumatoid nodules, severe extra-articular manifestations, and treatment with biologic in first year (Table 1). Risk factors for PE in RA included age, current and former smoking, BMI >30 kg/m2, rheumatoid nodules, large joint swelling, and treatment with biologic in first year. Remission in the first year was associated with lower PE risk (Table 2). Patients with RA were more likely to die following VTE (HR 1.52, 95%CI 1.04-2.21), adjusting for age, sex and year of VTE.
Conclusion: The risk of DVT and PE, and mortality following any VTE event were significantly increased in patients with RA vs non-RA. Several RA disease characteristics were associated with increased risk of DVT and PE. Remission was associated with reduced PE risk, underscoring benefits of tight control of RA disease activity. Despite recent RA treatment advancements, the risk of VTE in RA did not decline after 2000s, like the non-RA population trends. Better understanding of these indicators presents future research areas to improve care of patients with RA at risk of VTE.
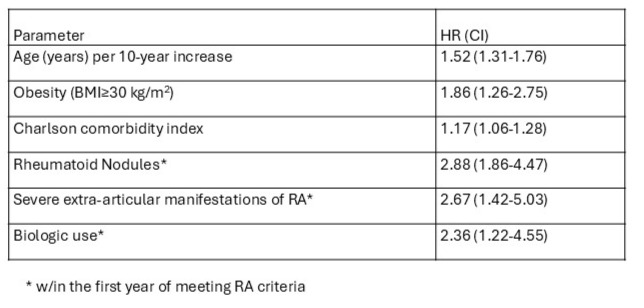 Table 1. Risk factors for DVT in patients with RA
Table 1. Risk factors for DVT in patients with RA
.jpg) Table 2. Risk factors for PE in patients with RA
Table 2. Risk factors for PE in patients with RA
To cite this abstract in AMA style:
Frechette N, myasoedova E, Javed I, George R, Achenbach S, Crowson C. Trends In Incidence and Risk factors For Incident Venous Thromboembolism in Patients with Rheumatoid Arthritis: A Population-Based Retrospective Cohort Study [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/trends-in-incidence-and-risk-factors-for-incident-venous-thromboembolism-in-patients-with-rheumatoid-arthritis-a-population-based-retrospective-cohort-study/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/trends-in-incidence-and-risk-factors-for-incident-venous-thromboembolism-in-patients-with-rheumatoid-arthritis-a-population-based-retrospective-cohort-study/