Session Information
Session Type: Poster Session B
Session Time: 9:00AM-10:30AM
Background/Purpose: Kidney biopsy is a gold standard for diagnosis and prognostication of lupus nephritis (LN). While interstitial fibrosis and tubular atrophy (IFTA) predict progression to chronic kidney disease (CKD), current NIH classification of interstitial inflammation only assesses for inflammation in unscarred cortical parenchyma and is found not predictive of CKD progression. The objective of this study was to determine whether total interstitial inflammation that accounts for inflammation in the entire cortical parenchyma in areas with and without fibrosis could predict CKD progression in patients with LN. Early identification of at-risk patients and combination therapies may improve outcomes.
Methods: A retrospective cohort study included 125 SLE patients with LN class III, IV, V or mixed (III/V, IV/V) on the index biopsy (2005-2018). Renal biopsies were reviewed and assigned based on the 2018-NIH Activity Index/Chronicity Index, and tubulointerstitial lesion categories. Total interstitial inflammation in the entire cortical parenchyma (ti score) was graded as 0, 1, 2, and 3 corresponding to < 10%, 10-25%, 26-50%, and >50% of the total cortical parenchyma containing an inflammatory infiltrate (similar to the definition used in the Banff ti score). CKD progression was defined as an estimated glomerular filtration rate (eGFR) decline by ≥30% within 5 years post-index biopsy. Parallel time-dependent analyses were performed to determine whether the total intestinal inflammation score and NIH interstitial inflammation score predict CKD progression.
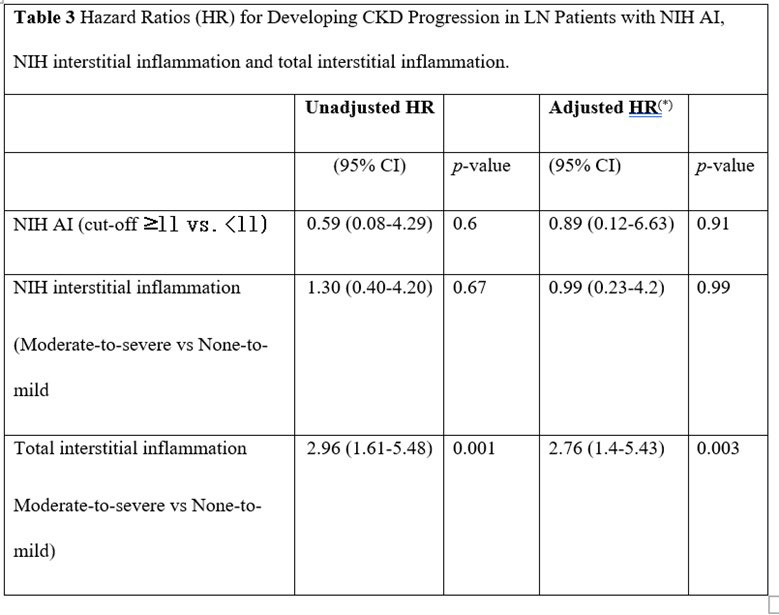
Results: Of 125 patients, 46 developed CKD progression. There were no differences in baseline characteristics between progressors and non-progressors (Table 1). Of these patients, 28 (22.4%) had moderate-to-severe total interstitial inflammation and 8 (6.4%) had moderate-to-severe NIH interstitial inflammation (Table 2). Total interstitial inflammation was associated with CKD progression in bivariate and time-dependent analyses [HR (95%CI): 2.76 (1.4-5.43) adjusted for age at biopsy, race and sex)]. NIH interstitial inflammation was not associated with CKD progression (Table 3).
Conclusion: Accounting for interstitial inflammation in the entire cortical parenchyma in areas with and without fibrosis identifies patients at risk for CKD progression.
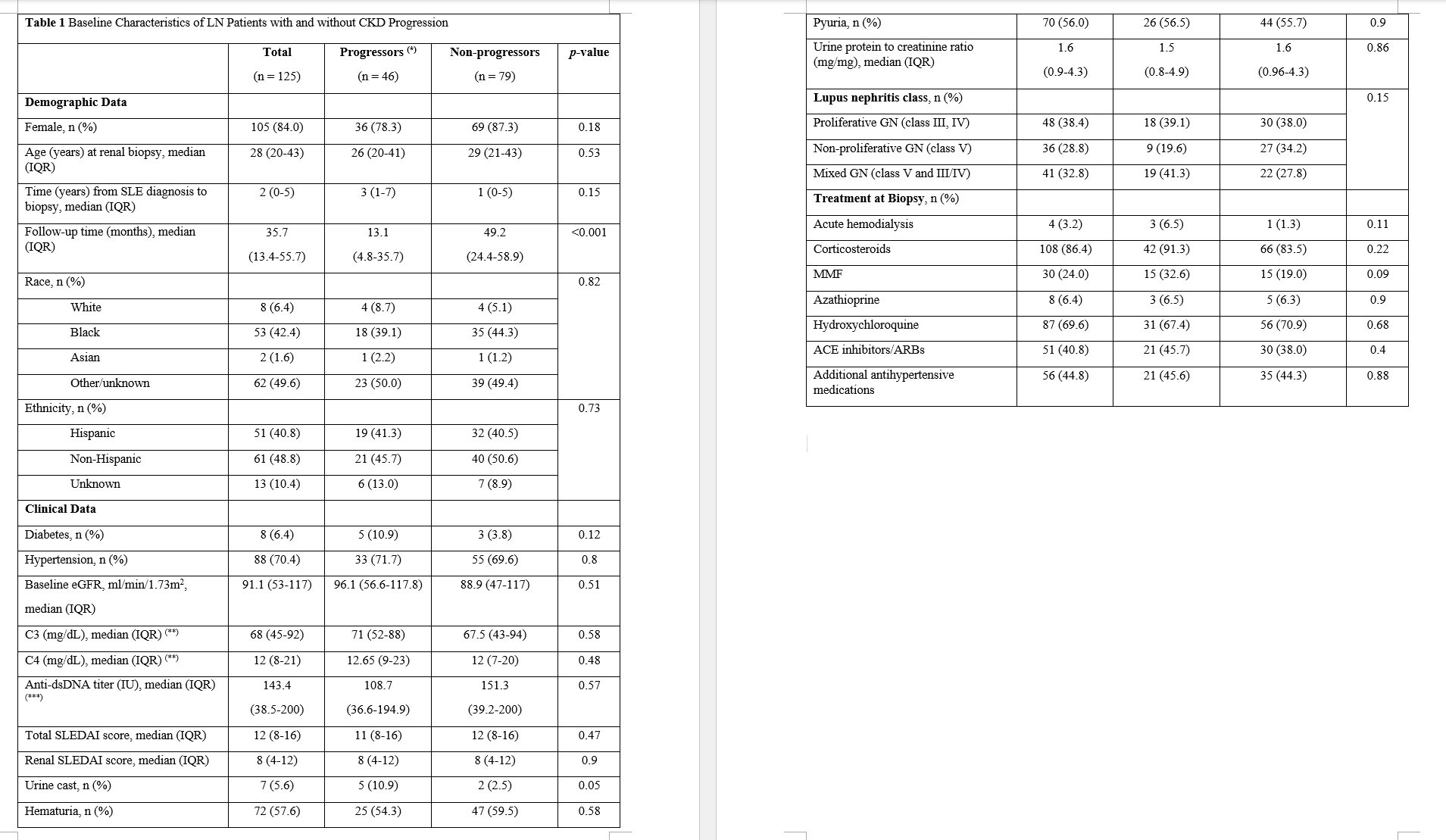
Abbreviations: CKD, chronic kidney disease; SLE, systemic lupus erythematosus; SLEDAI, SLE disease activity index; GN, glomerulonephritis; MMF, mycophenolate mofetil; ACE, angiotensin converting enzyme; ARBs, angiotensin receptor blockades.
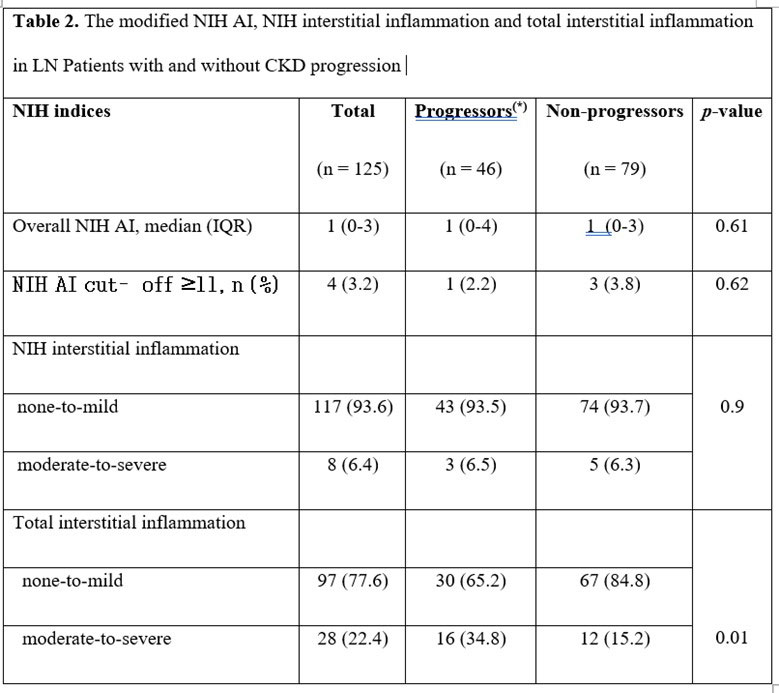
Abbreviations: NIH, National Institutes of Health; AI, activity index.
To cite this abstract in AMA style:
Duong M, Wang S, Schwartz D, Mowrey W, Broder A, Goilav B. Total Interstitial Inflammation Predicts Chronic Kidney Disease Progression in Patients with Lupus Nephritis [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/total-interstitial-inflammation-predicts-chronic-kidney-disease-progression-in-patients-with-lupus-nephritis/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/total-interstitial-inflammation-predicts-chronic-kidney-disease-progression-in-patients-with-lupus-nephritis/