Session Information
Date: Monday, October 27, 2025
Title: (1123–1146) Metabolic & Crystal Arthropathies – Basic & Clinical Science Poster I
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: CPPD has been associated with osteopenia of the metacarpal heads and a 2x increased risk for fracture of the wrist, hip, humerus or pelvis. Inorganic pyrophosphate is a known strong inhibitor of mineralization and a critical component of calcium pyrophosphate crystals. We conducted a pilot study testing for differences in tibial bone microstructure and histomorphometry in CPPD vs. controls.
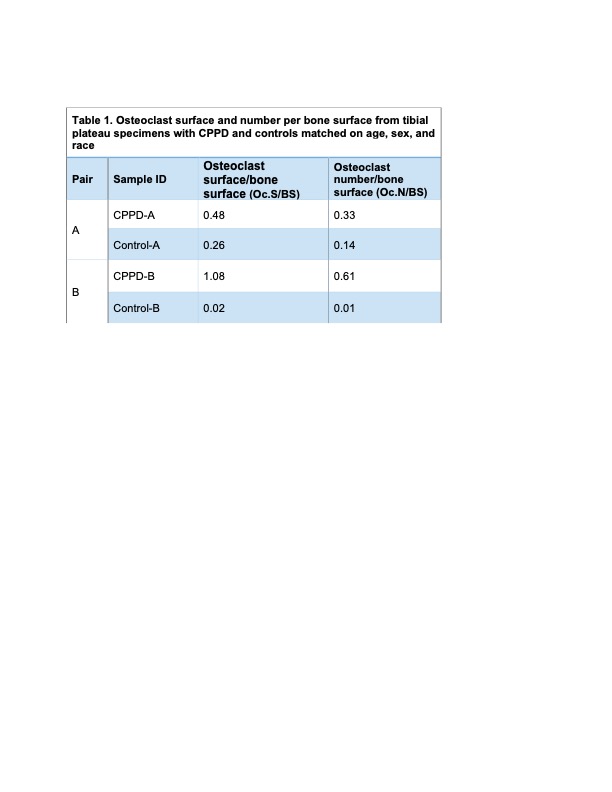
Methods: Among patients undergoing total knee replacement surgery at a single academic medical center, we reviewed pre-operative radiographs for the presence of chondrocalcinosis in the knee, which defines the CPPD cohort. For each CPPD patient we identified one control matched on age (+/-5 years), sex, and race; controls were defined by absence of chondrocalcinosis on any joint radiograph. The tibial compartment analyzed (lateral or medial) was the same for each pair and was defined by the location of chondrocalcinosis in the CPPD patient and absence of Kellgren-Lawrence grade 4 in that compartment in both CPPD patients and controls. Microcomputed tomography (microCT) scanning was performed on formalin-fixed samples using a Scanco Medical mCT35 scanner with an isotropic voxel size of 20mm. A semi-automated contouring approach was used to exclude cortical bone and bone volume/tissue volume was calculated using software supplied by the manufacturer and a global threshold that set the bone/marrow cut-off at 398mg HA/cm3. Following decalcification and paraffin-embedding, trabeculae in the subchondral region were traced using Osteomeasure to determine bone surface area. TRAP staining identified osteoclasts (Oc) and Safranin O staining highlighted articular cartilage. Mean Oc surface/bone surface (Oc.S/BS) and Oc number/BS (Oc.N/BS) were calculated from 3 segments per sample.
Results: We obtained samples from 5 CPPD-control pairs (4 lateral compartment pairs, 1 medial compartment pair). Mean age was 69.6 (SD 9.5) years, 2 pairs were female, and all were White. Tibial plateau BV/TV was lower in samples from individuals with CPPD than controls (p=0.09) (Figure 1). Histomorphometry was performed for 2 pairs; analysis of the 3 remaining pairs is ongoing. Oc.S/BS and Oc.N/BS were higher in tibial plateau subchondral trabecular bone from individuals with CPPD than controls (Table 1, Figure 2).
Conclusion: Tibial plateau trabecular bone had lower BV/TV and more abundant osteoclasts in knee compartments with chondrocalcinosis among patients undergoing knee replacement surgery. These preliminary findings are directionally consistent with prior cohort studies that reported a greater risk of osteopenia and fractures in CPPD, and suggest a link between localized inorganic pyrophosphate and compromised bone microstructure.
.jpg)
.jpg)
To cite this abstract in AMA style:
Tedeschi S, Kushwaha P, Gill M, Charles J, Gravallese E. Tibial Bone Microstructure and Histomorphometry in Individuals with CPPD [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/tibial-bone-microstructure-and-histomorphometry-in-individuals-with-cppd/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/tibial-bone-microstructure-and-histomorphometry-in-individuals-with-cppd/