Session Information
Date: Monday, November 14, 2022
Title: SLE – Diagnosis, Manifestations, and Outcomes Poster III: Outcomes
Session Type: Poster Session D
Session Time: 1:00PM-3:00PM
Background/Purpose: An important clinical question is whether treatments (e.g, corticosteroids, immunosuppressants) or SLE disease activity are associated with an increased risk of COVID-19 infection among SLE patients. We analyzed data from a large cohort of patients with SLE to assess the association between demographic, clinical, and immunologic characteristics and incident COVID-19 infection.
Methods: The study was based on data from a large cohort of SLE patients seen quarterly. We merged in information on COVID-19 infection, vaccination history, and COVID-19 antibodies. The risk of acquisition of COVID-19 in any month of follow-up after March 1, 2020 was estimated as a function of the demographic and clinical characteristics of the patient assigned to that month of follow-up based on cohort information. For those vaccinated, SARS-CoV-2 IgG was measured by ELISA (Euroimmun).
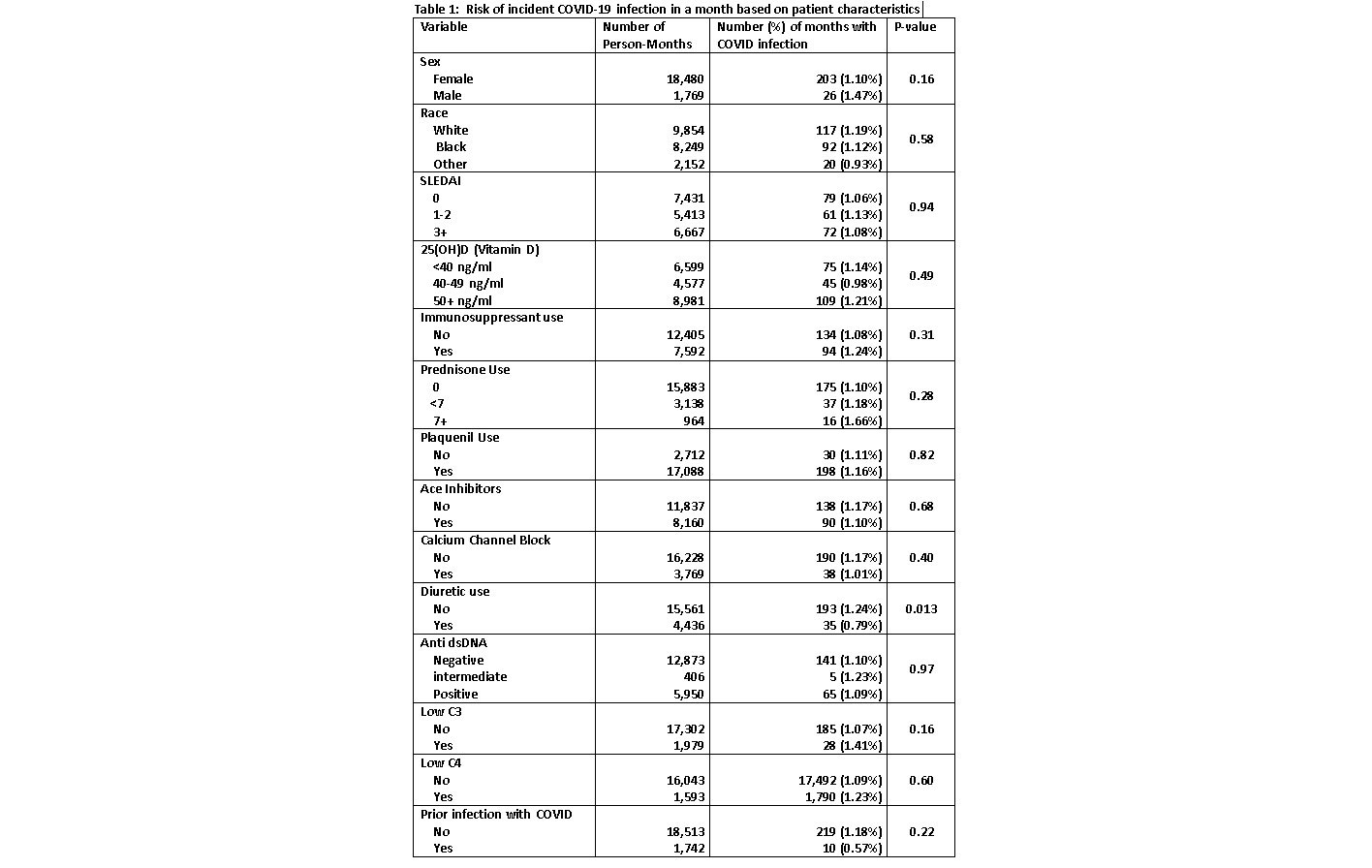
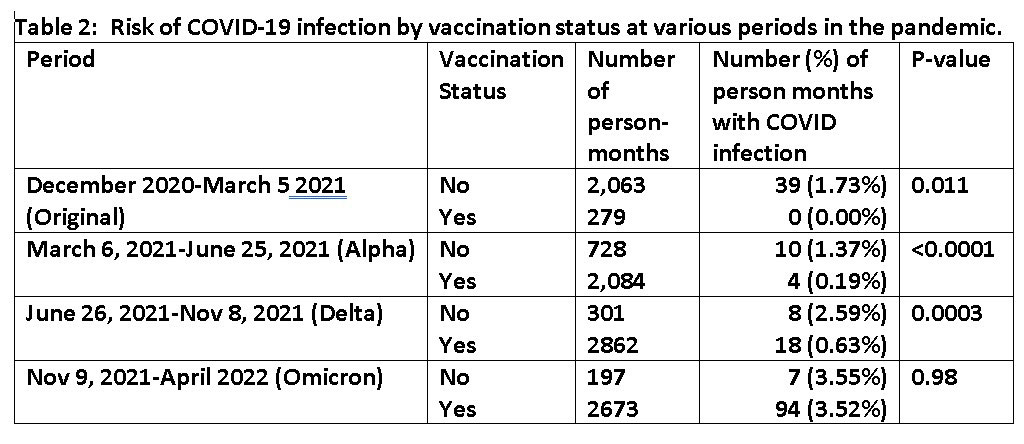
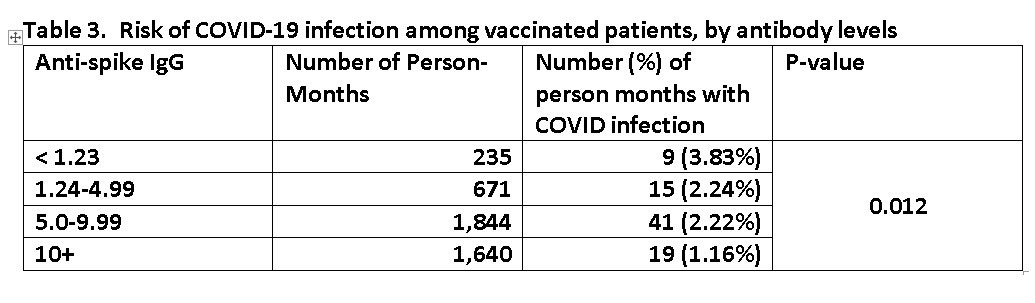
Results: The analysis was based on 20,255 person-months from 1017 different patients. There were 229 incident cases of COVID experienced by 219 patients. Table 1 shows the monthly risk of incident COVID based on patient demographic and clinical characteristics. There was not an increased risk of infection among those on corticosteroids, immunosuppressants, or those with higher levels of disease activity. Table 2 shows the relationship between vaccination status and risk of COVID-19 infection based on follow-up that occurred after December 2020. This analysis excludes follow-up that occurred after a patient was infected with COVID. Those vaccinated had a significantly lower risk of infection during all phases of the epidemic except the most recent phase where risks were similar between vaccinated and unvaccinated. Table 3 shows the relationship between recent antibody levels and risk of infection. Higher antibody levels were associated with a lower risk, and there does not appear to be a threshold that confers maximum protection.
Conclusion: It is reassuring that typical SLE treatments and SLE disease activity do not seem to be associated with a higher risk of incident COVID-19 infection. In this cohort, vaccination did not appear to be protective against infection in the current (Omicron) phase of the epidemic. Importantly, the higher a person’s antibody levels, the better protection they have.
To cite this abstract in AMA style:
Magder L, Fava A, Goldman D, Petri M. The Incidence of COVID-19 Infection in an SLE Cohort, and Its Association with Immunosuppressants, SLE Disease Activity, Vaccination Status, and COVID-19 Antibodies [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/the-incidence-of-covid-19-infection-in-an-sle-cohort-and-its-association-with-immunosuppressants-sle-disease-activity-vaccination-status-and-covid-19-antibodies/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-incidence-of-covid-19-infection-in-an-sle-cohort-and-its-association-with-immunosuppressants-sle-disease-activity-vaccination-status-and-covid-19-antibodies/