Session Information
Date: Monday, November 8, 2021
Title: Epidemiology & Public Health Poster III: Other Rheumatic & Musculoskeletal Diseases (1022–1060)
Session Type: Poster Session C
Session Time: 8:30AM-10:30AM
Background/Purpose: Musculoskeletal (MSK) disorders, including low back pain and osteoarthritis (OA), are ranked among the top causes of years lived with disability and increased risk-attributable disability-adjusted life-years. ELSA-Brasil MSK is an ancillary study of the ELSA-Brasil that investigates the incidence and risk factors for MSK disorders. Here we briefly describe the design and implementation of the cohort and presented prevalence of chronic musculoskeletal pain (CMP) and knee OA at baseline.
Methods: ELSA-Brasil MSK includes active and retired civil servants from one of the investigation centers (IC) of ELSA-Brasil (IC-Minas Gerais) who completed assessments on five different domains concerning MSK health (rheumatic diseases and symptoms; disability and physical functioning; mechanical risk factors; personal beliefs; care seeking) at study baseline (2012-2014). Cohort surveillance has been performed through annual telephone interviews and return visits (scheduled every 4 years after enrollment), collecting extensive information on exposures, subclinical and clinical outcomes. A total of 2,901 participants were assessed for CMP (≥ 6 months in the past year) at nine body sites: neck, shoulders, upper back, elbows, lower back, wrists/hands, hips/thighs, knees, ankles/feet. CMP was described as multisite ( >3 sites) and generalized (3 regions: upper + lower limbs + axial skeleton). 2,830 participants underwent hand and/or knee radiography for the diagnosis of OA along with the assessment of frequent hand/knee pain (pain on most days of at least 1 month). Radiographic knee OA (RKOA) was defined as the presence of tibiofemoral (TF) (KL ≥2) and/or patellofemoral (PF) (definitive osteophyte ≥2 or joint space narrowing ≥2 +bone abnormality) OA and symptomatic knee OA (SKOA) as the presence of RKOA + frequent knee pain in the corresponding knee.
Results: Participants were aged between 38 and 79 years old (mean 56.0 SD 8.9), 52.9% were women. CMP in at least one site was observed in 55.1% of participants and there was a high prevalence of multisite (19.1%) and generalized (10.3%) CMP. CMP was more commonly observed among females and participants who were older, non-white, less educated, retired, with depression, and those with higher body mass index and number of comorbidities (Table 1). The prevalence RKOA and SKOA was 18.1% and 7.8%, respectively. TF compartment was scored as KL in 2 in 7.6%, 3 in 3.0% and 4 in 1.1% of 5,638 knee images (Table 2). Most knees with RKOA (n=740) showed isolated TF OA (56.6%), with isolated PF OA in 11.4% of knees (Figure 1).
Conclusion: The high prevalence of CMP and knee OA indicates a large burden of MSK disorders in Brazil. Future longitudinal analyses in ELSA-Brasil MSK will provide an unique opportunity to fill current knowledge gaps about psychosocial and biological determinants of these disorders in a middle-income country.
Funding: ELSA-Brasil is supported by the Brazilian Ministry of Health and of Science and Technology (FINEP and CNPq-BR), (Grants 01 06 0010.00 RS, 01 06 0212.00 BA, 01 06 0300.00 ES, 01 06 0278.00 MG, 01 06 0115.00 SP, 01 06 0071.00 RJ). ELSA-Brasil MSK has been supported by CAPES-BR (054/2010), FAPEMIG-BR (APQ-00921-16) and CNPq-BR (42358520169).
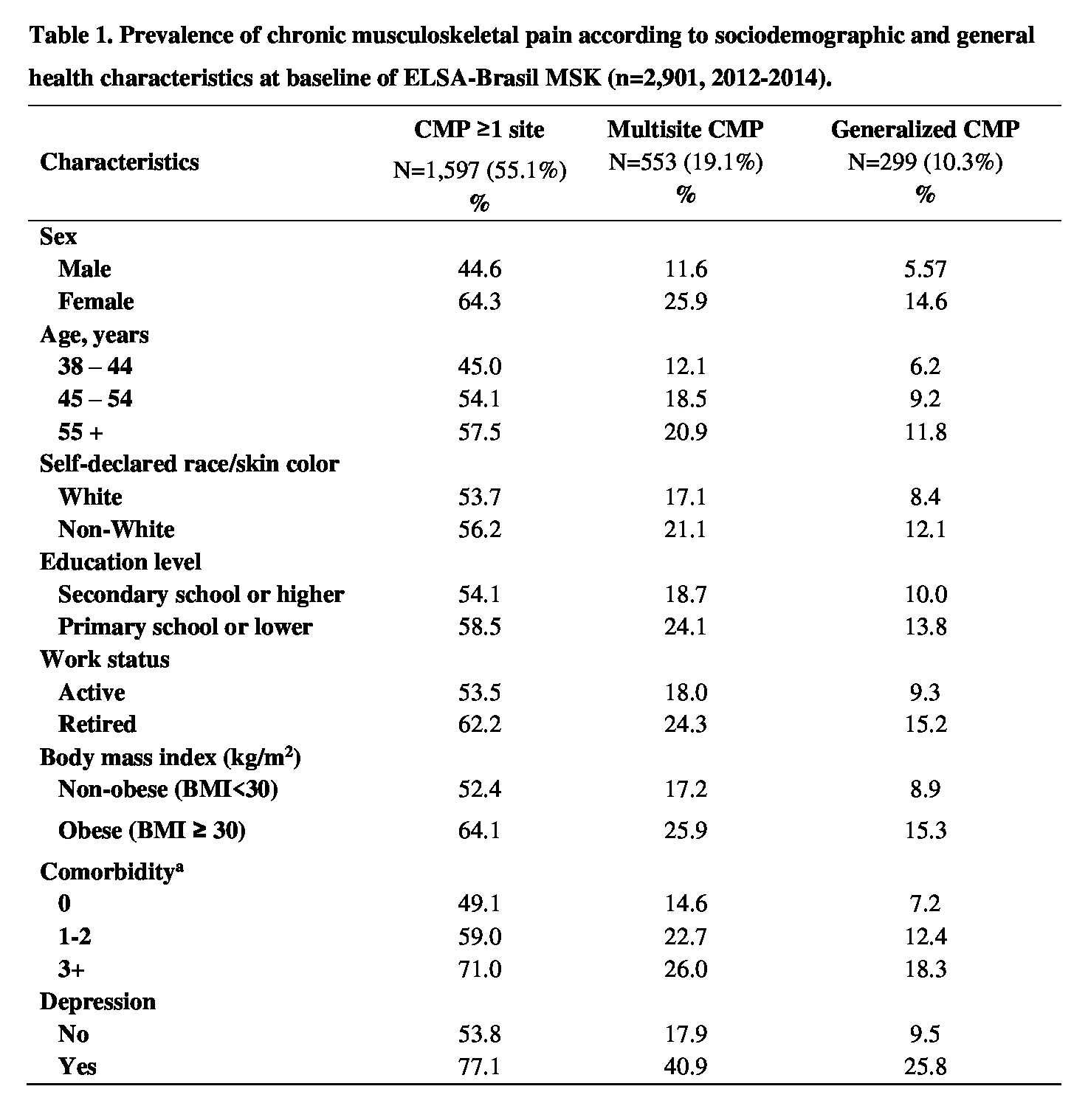 BMI, body mass index. MSK, musculoskeletal. CMP, chronic musculoskeletal pain. CLBP, chronic low back pain. aComorbidity: hypertension, diabetes, myocardial infarction, heart failure, stroke, kidney disease, COPD, cirrhosis, cancer.
BMI, body mass index. MSK, musculoskeletal. CMP, chronic musculoskeletal pain. CLBP, chronic low back pain. aComorbidity: hypertension, diabetes, myocardial infarction, heart failure, stroke, kidney disease, COPD, cirrhosis, cancer.
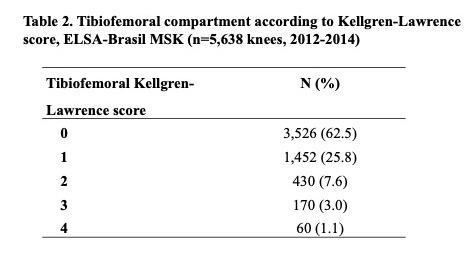
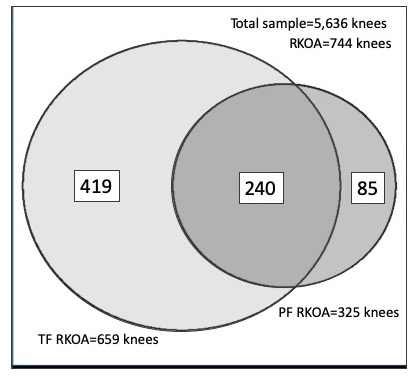 Figure 1 Venn Diagram of radiographic OA in ELSA-Brasil MSK (n=5,636 knees*, 2012_2014) *n=5,636 knees tibiofemoral and patellofemoral radiographic images
Figure 1 Venn Diagram of radiographic OA in ELSA-Brasil MSK (n=5,636 knees*, 2012_2014) *n=5,636 knees tibiofemoral and patellofemoral radiographic images
To cite this abstract in AMA style:
Weiss Telles R, Machado L, Costa-Silva L, Maria Barreto S. The ELSA-Brasil Musculoskeletal Cohort (ELSA-Brasil MSK): Design, Implementation and Prevalence of Chronic Musculoskeletal Pain and Radiographic Knee Osteoarthritis at Baseline [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/the-elsa-brasil-musculoskeletal-cohort-elsa-brasil-msk-design-implementation-and-prevalence-of-chronic-musculoskeletal-pain-and-radiographic-knee-osteoarthritis-at-baseline/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-elsa-brasil-musculoskeletal-cohort-elsa-brasil-msk-design-implementation-and-prevalence-of-chronic-musculoskeletal-pain-and-radiographic-knee-osteoarthritis-at-baseline/