Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Uncontrolled gout (UG) is a chronic, progressive, and systemic disease characterized by serum uric acid (sUA) >6 mg/dl and clinical manifestations such as tophi, flares and gouty arthropathy, despite the use of urate lowering therapy (ULT). Limited real-world evidence exists on the UG care pathway from diagnosis to long-term management. This study examined the care pathway and treatment patterns of patients with UG in the United States (US).
Methods: Data were extracted from the Adelphi Real World Gout Disease Specific Programme™, a cross-sectional survey, with retrospective data collection, of physicians (rheumatologists, nephrologists and primary care physicians [PCPs]) and their patients with gout in the US between August 2023 – March 2024. Physicians who participated in the study managed ≥8 patients with gout a month. UG was defined as sUA >6 mg/dl and at least one of the following: gouty arthropathy, ≥1 tophi, or ≥2 flares in the 12 months prior. Patients had to be receiving a ULT. Physicians reported patient demographics, treatment patterns, care pathway and clinical manifestations such as sUA levels, number of tophi and signs/symptoms at diagnosis, treatment initiation and data collection. All patients had a known treatment duration. Analyses were descriptive.
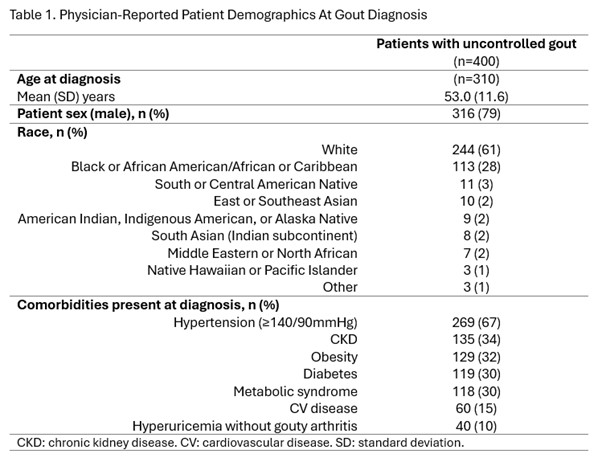
Results: Overall, 88 physicians (45 rheumatologists, 22 nephrologists and 21 PCPs) reported data for 400 patients with UG. In patients who developed UG, there was a mean (standard deviation, SD) of 0.4 (1.3) years between a patients’ first physician visit and gout diagnosis. At diagnosis mean (SD) patient age (n=310) was 53.0 (11.6) years, sUA level (n=330), number of tophi (n=173), and signs/symptoms (n=369) were 11.7 (4.7) mg/dL, 2.8 (2.9), and 2.7 (1.8), respectively.At initiation of current treatment (n=400), mean (SD) sUA level, number of tophi and signs/symptoms were 10.8 (4.3) mg/dL, 3.7 (3.3) and 3.1 (1.9), respectively. Rheumatologists prescribed the current treatment in 56% of patients, nephrologists 29% and PCPs 12%. The most common ULT was allopurinol (63%), followed by febuxostat (29%) and pegloticase (13%). The most common reasons reported by physicians for choosing the current treatment were overall efficacy, long-term efficacy, and sUA reduction for 86%, 63%, and 54% of patients, respectively. However, these same characteristics were also reported by physicians as the most common areas where the treatments could perform better in 32%, 27%, 25% of patients respectively.At data collection (n=400), after a mean (SD) of 21.2 (25.6) months on the current ULT, mean (SD) sUA level, number of tophi and signs/symptoms were 9.1 (4.3) mg/dL, 2.9 (3.1) and 2.7 (1.8), respectively. Mean (SD) number of flares (n=357) in the 12 months prior was 2.3 (1.1).
Conclusion: To our knowledge, this is the first real-world study examining the care pathway and treatment patterns of patients with UG. These data highlight that patients with UG experience extended periods of time with elevated sUA and UG clinical manifestations, despite receiving ULT for almost two years. Given that efficacy was noted as the most common reason for treatment choice and area of improvement, there is a need for optimal treatment utilization and alternative options for patients with UG.
.jpg) GP: general practitioner, PCP: Primary care physician, SD: standard deviation, sUA: serum urate acid. Other physicians include ER physician, Podiatrist, Nurse / nurse practitioner, Orthopaedic Surgeon, Other physician. Possible signs/symptoms: Cramp, Fatigue, Fever/flu like symptoms, Gouty arthropathy, defined clinically or radiographically as joint damage due to gout, High sUA (> 6mg/dL), Joint stiffness, Loss of movement/loss of mobility, Pain between flares (chronic pain), Sleep disturbance, Tender/swollen joint(s), Visible tophus(i), Warm joints, Other, None
GP: general practitioner, PCP: Primary care physician, SD: standard deviation, sUA: serum urate acid. Other physicians include ER physician, Podiatrist, Nurse / nurse practitioner, Orthopaedic Surgeon, Other physician. Possible signs/symptoms: Cramp, Fatigue, Fever/flu like symptoms, Gouty arthropathy, defined clinically or radiographically as joint damage due to gout, High sUA (> 6mg/dL), Joint stiffness, Loss of movement/loss of mobility, Pain between flares (chronic pain), Sleep disturbance, Tender/swollen joint(s), Visible tophus(i), Warm joints, Other, None
To cite this abstract in AMA style:
Lam G, Bhor M, Hawthorne J, Dada A, Edwards M, Goddard E, Albert J. The Care Pathway and Treatment Patterns in Patients with Uncontrolled Gout: A Real-World Survey of Physicians In The United States [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/the-care-pathway-and-treatment-patterns-in-patients-with-uncontrolled-gout-a-real-world-survey-of-physicians-in-the-united-states/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-care-pathway-and-treatment-patterns-in-patients-with-uncontrolled-gout-a-real-world-survey-of-physicians-in-the-united-states/