Session Information
Session Type: Poster Session A
Session Time: 8:30AM-10:30AM
Background/Purpose: Physical activity is a potential target for interventions in knee OA. However, most of the available studies concerning physical activity in individuals with knee OA were performed in relatively old populations with an inactive lifestyle. It is unclear how previous results can be generalized to other populations with different lifestyle and physical activity habits.
Therefore, we investigated if knee OA is associated with lower physical activity in a general middle-aged Dutch population. Furthermore, we investigated the association of physical activity with patient reported outcomes such as knee pain and function, and health-related quality of life in individuals with knee OA.
Methods: We used cross-sectional data from the Netherlands Epidemiology of Obesity (NEO) study, in which participants aged 45-65 years were included. Clinical knee OA was defined using the criteria by Altman et al. Structural knee OA was defined on MRI using the modified criteria by Hunter et al. in a random subset of 1,285 individuals of our study population.
We assessed knee pain and function with the Knee injury and Osteoarthritis Score (KOOS), and health-related quality of life (HRQoL) with the Short Form (SF)-36. Physical activity (in Metabolic Equivalent of Task (MET) hours per week) was assessed using the Short Questionnaire to Assess Health-enhancing physical activity (SQUASH).
We used linear regression analyses to investigate 1) the association of knee OA with physical activity, and 2) of physical activity with knee pain, function, and HRQoL in participants with clinical knee OA. All analyses were adjusted for age, sex, body mass index (BMI), ethnicity, educational level and comorbidities. To account for possible information bias, we performed a sensitivity analysis to assess the association between clinical knee OA and physical activity measured by an accelerometer in a random subset of 15% of the study population.
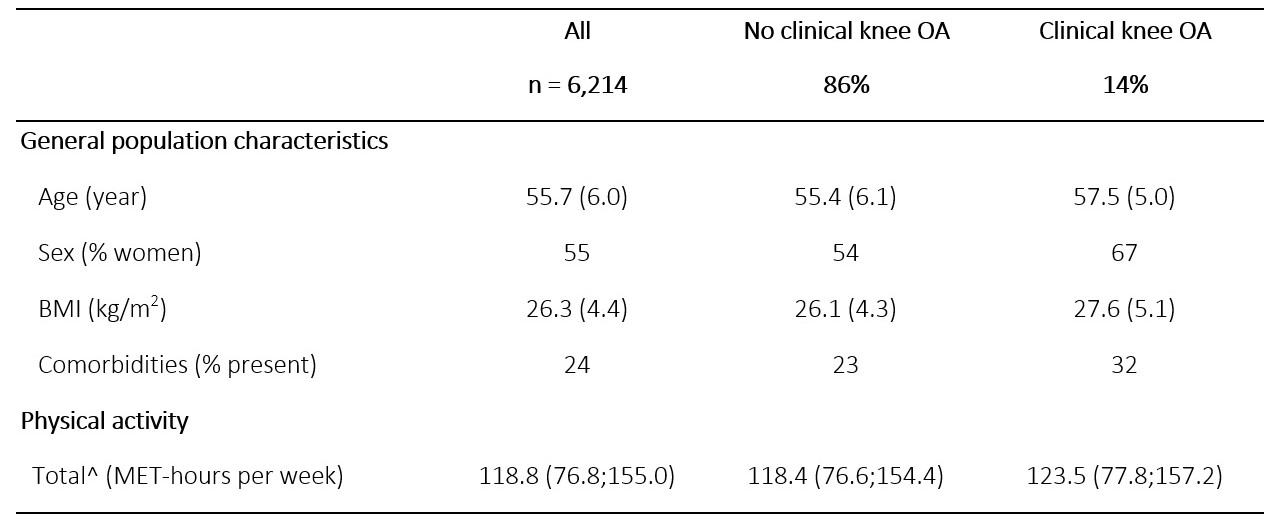
Results: Of 6,212 participants, we observed clinical knee OA in 14%, and structural knee OA in 12%. The general population characteristics and median physical activity of our study population are presented in table 1. In comparison to participants without knee OA, participants with clinical knee OA had on average 9.60 (95% CI 3.70;15.50) MET hours per week more total physical activity (figure 1). Structural knee OA was associated with 3.97 (-7.82; 15.76) MET hours per week more physical activity, compared with no structural knee OA.
Sensitivity analysis showed a weak positive association of clinical knee OA with physical activity measured by an accelerometer: 2.37 (-6.05; 10.80) MET hours per week more physical activity was found in participants with clinical knee OA, compared with participants without clinical knee OA. In the subpopulation of participants with clinical knee OA, physical activity was not associated with knee pain, function or HRQoL.
Conclusion: Knee OA was not associated with lower physical activity in this middle-aged Dutch population. Future research should indicate the optimal treatment advice regarding physical activity for individual knee OA patients.

To cite this abstract in AMA style:
Terpstra S, van der Velde J, de Mutsert R, Schiphof D, Reijnierse M, Rosendaal F, van de Stadt L, Kloppenburg M, Loef M. The Association of Clinical and Structural Knee Osteoarthritis with Physical Activity in the Middle-aged Population: The Netherlands Epidemiology of Obesity Study [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/the-association-of-clinical-and-structural-knee-osteoarthritis-with-physical-activity-in-the-middle-aged-population-the-netherlands-epidemiology-of-obesity-study/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-association-of-clinical-and-structural-knee-osteoarthritis-with-physical-activity-in-the-middle-aged-population-the-netherlands-epidemiology-of-obesity-study/