Session Information
Date: Sunday, November 12, 2023
Title: (0229–0251) Metabolic & Crystal Arthropathies – Basic & Clinical Science Poster I
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Recurrent flares are the hallmark of clinical manifestation of gout. Sodium-glucose cotransporter-2 inhibitors (SGLT2i) were associated with a lower risk of incident gout; however, their impact on recurrent flares is unknown. We aimed to examine the relation of SGLT2i vs. active comparators (i.e., glucagon-like peptide-1 receptor agonist or dipeptidyl peptidase 4 inhibitors) to the risk of recurrent gout flares, the first recurrent gout flare, and all-cause mortality among patient with gout and type 2 diabetes.
Methods: Using IQVIA Medical Research Database in the United Kingdom, we identified initiators of SGLT2i and active comparators among gout patients with type 2 diabetes from a United Kingdom primary care database. We conducted cohort studies to examine the relation of SGLT2i vs. active comparators to the risk of recurrent flares, the first recurrent flare, and all-cause mortality using either Poisson regression or Cox-proportional hazards model with propensity score overlap weighting. The primary outcome was the number of recurrent gout flares that were ascertained using recorded codes and prescriptions records. Secondary outcomes were the first recurrent gout flare and all-cause mortality.
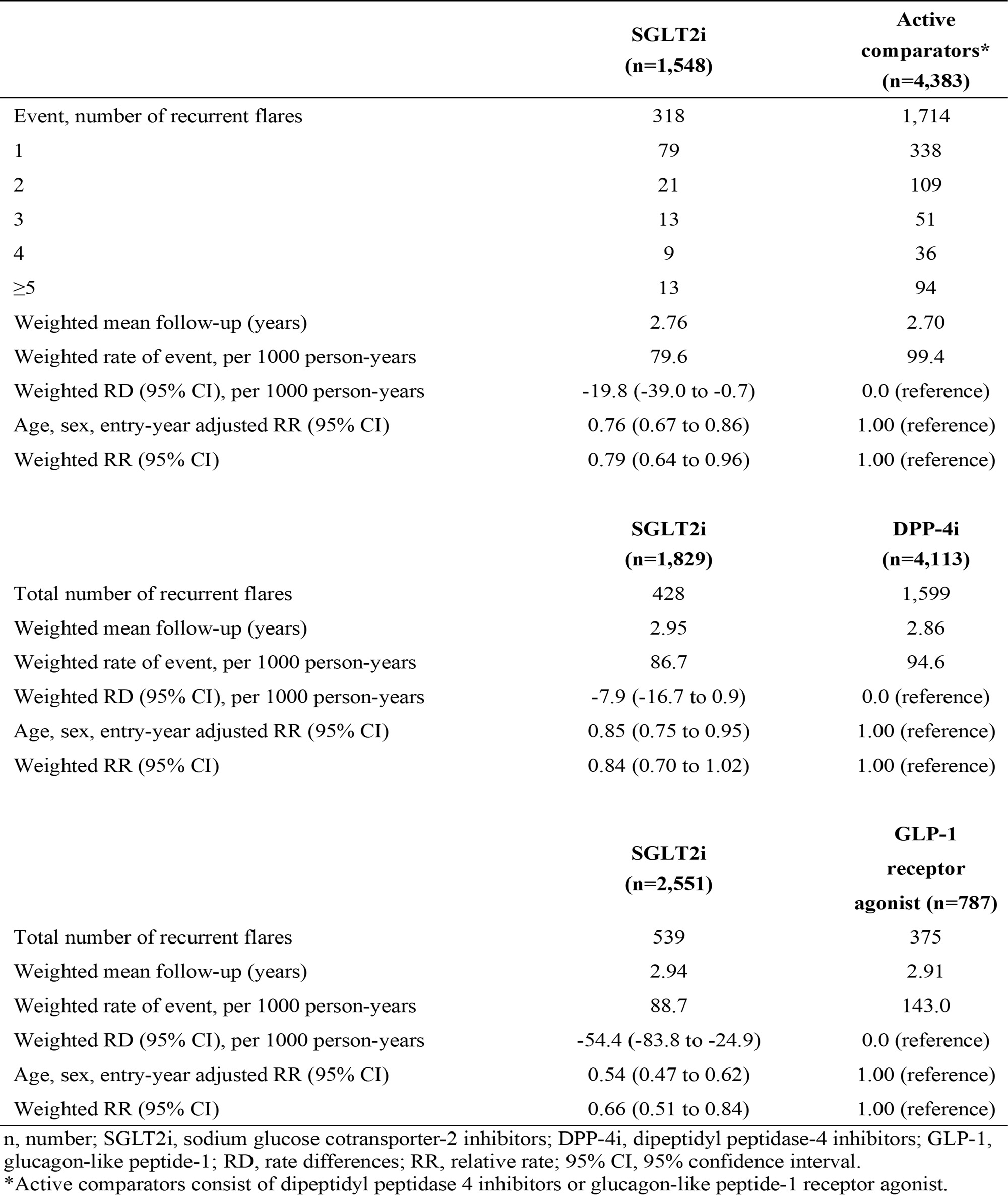
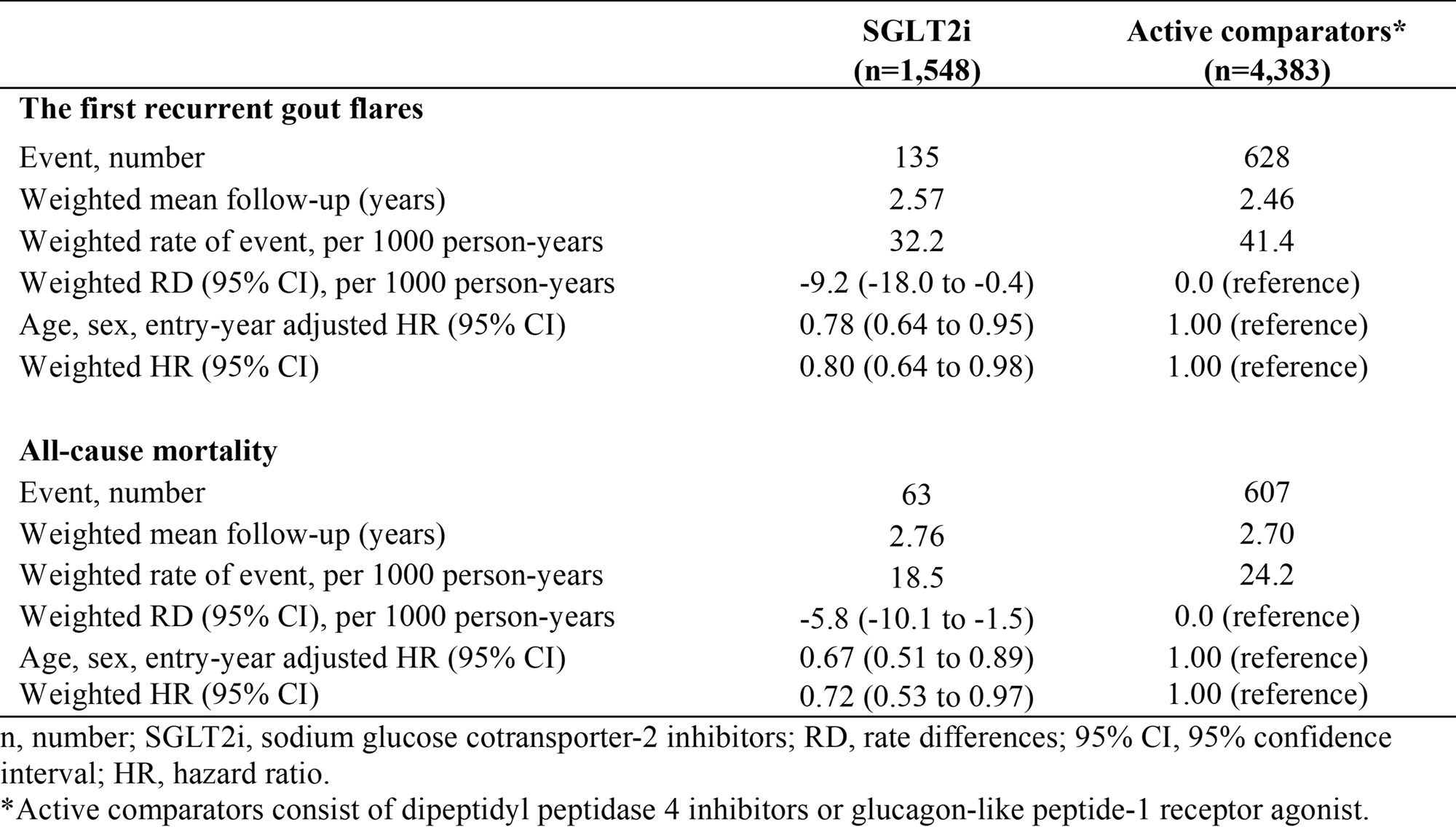
Results: During 17,729 person-years of follow-up, 318 recurrent flares occurred in the 1,548 initiators of SGLT2i and 1,714 in the 4,383 initiators of active comparators, respectively. The relative rate of the recurrent flares of SGLT2i vs. active comparators was 0.79 (95%CI: 0.64 to 0.96). Similar results were observed in the relation of SGLT2i to the risk of number of recurrent flares when compared with DPP-4i or GLP-1 receptor agonist, respectively (Table 1). The rate difference (RD) and hazard ratio (HR) of the first recurrent flare for SGLT2i vs. active comparators were -9.2 (95%CI: -18.0 to -0.4) per 1000 person-years and 0.80 (95%CI: 0.64 to 0.98), respectively. All-cause mortality per 1000 person-years was 18.5 for SGLT2i and 24.2 for active comparators, with RD and HR being -5.8 (95%CI: -10.1 to -1.5) per 1000 person-years and 0.72 (95%CI: 0.53 to 0.97) (Table 2).
Conclusion: SGLT2i were associated with a lower risk of recurrent gout flares and mortality than their active comparators in patients with gout and type 2 diabetes. Our findings suggested that SGLT2i have a potential to reduce the burden of recurrent gout flares and narrow the mortality gap between patients with gout and the general population.
To cite this abstract in AMA style:
Wei J, Choi H, Dalbeth N, Li X, Li C, Zeng C, Lei G, Zhang Y. Sodium-glucose Cotransporter-2 Inhibitor Initiation, Risk of Recurrent Gout Flares, and Mortality in Patients with Gout and Type 2 Diabetes: A Population-based Cohort Study [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/sodium-glucose-cotransporter-2-inhibitor-initiation-risk-of-recurrent-gout-flares-and-mortality-in-patients-with-gout-and-type-2-diabetes-a-population-based-cohort-study/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/sodium-glucose-cotransporter-2-inhibitor-initiation-risk-of-recurrent-gout-flares-and-mortality-in-patients-with-gout-and-type-2-diabetes-a-population-based-cohort-study/