Session Information
Date: Sunday, November 13, 2022
Title: Abstracts: Miscellaneous Rheumatic and Inflammatory Diseases II
Session Type: Abstract Session
Session Time: 10:30AM-12:00PM
Background/Purpose: The inciting factor or antigen exposure that initiates sarcoidosis remains unknown. However, an infectious trigger such as Mycobacterium spp. or Propionibacterium acnes infection may play a role.
The Bacille Calmette-Guérin (BCG) vaccine is a live strain of Mycobacterium bovis developed to protect against tuberculosis (TB) and other mycobacterial infections. It also exerts additional benefits, such as protection against other respiratory illnesses and reduction in overall childhood mortality.
Denmark started a national BCG immunization program in 1946, during which time the vaccine was routinely administered to all children. This program precipitously declined in 1983 (affecting those born in 1976) and officially ended in 1986, due to a decrease in TB prevalence. Given the evidence for a potential infectious trigger of sarcoidosis (including Mycobacterium), and the protection and long-lasting trained immunity conferred by BCG vaccination, sarcoidosis rates may be reduced in BCG vaccinated patients.
Methods: We performed a registry-based incidence study on persons born between the years of 1970-1981 in Denmark using the Danish Civil Registration system and linked population health registries. We determined the incidence of sarcoidosis from 1995-2016 for people born between 1970-1981 based on ≥2 ICD-10 codes for sarcoidosis (D86) separated by ≥14 days. We calculated the incidence rate (IR) of sarcoidosis by birth year and sex. We used a Poisson model to calculate the incidence rate ratio (IRR) of sarcoidosis in BCG non-vaccinated vs vaccinated people, adjusting for birth year, age, and calendar year. BCG vaccination status was assigned based on birth year: people born before 1976 were very likely to receive the BCG vaccine and people born in or after 1976 were very unlikely to receive the BCG vaccine.
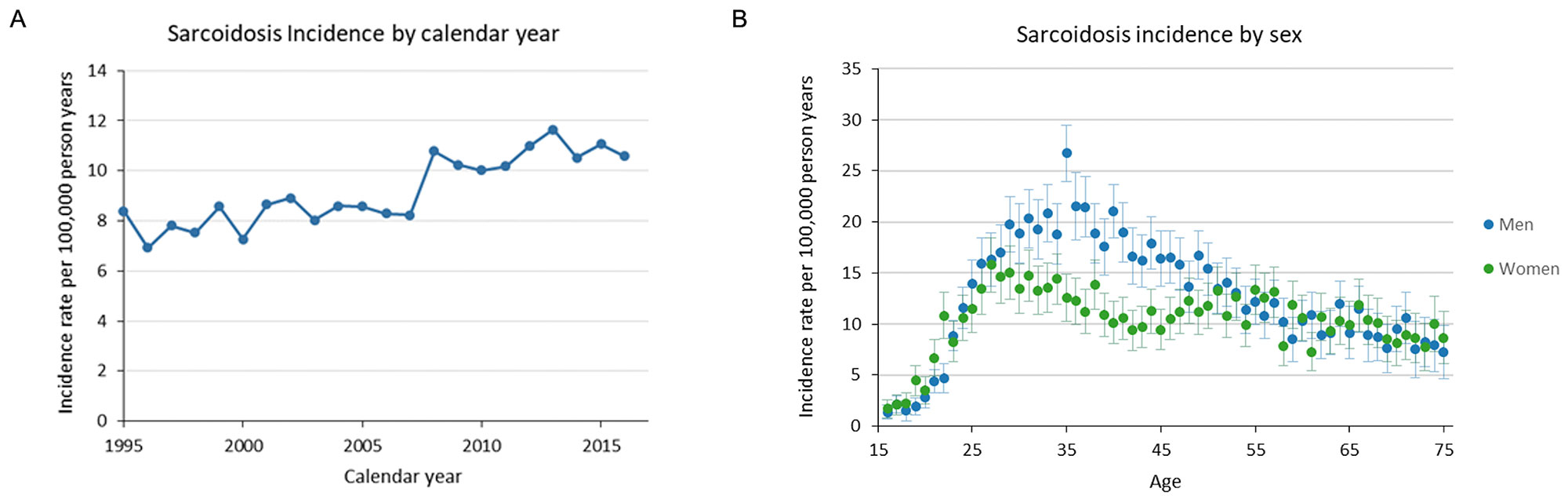
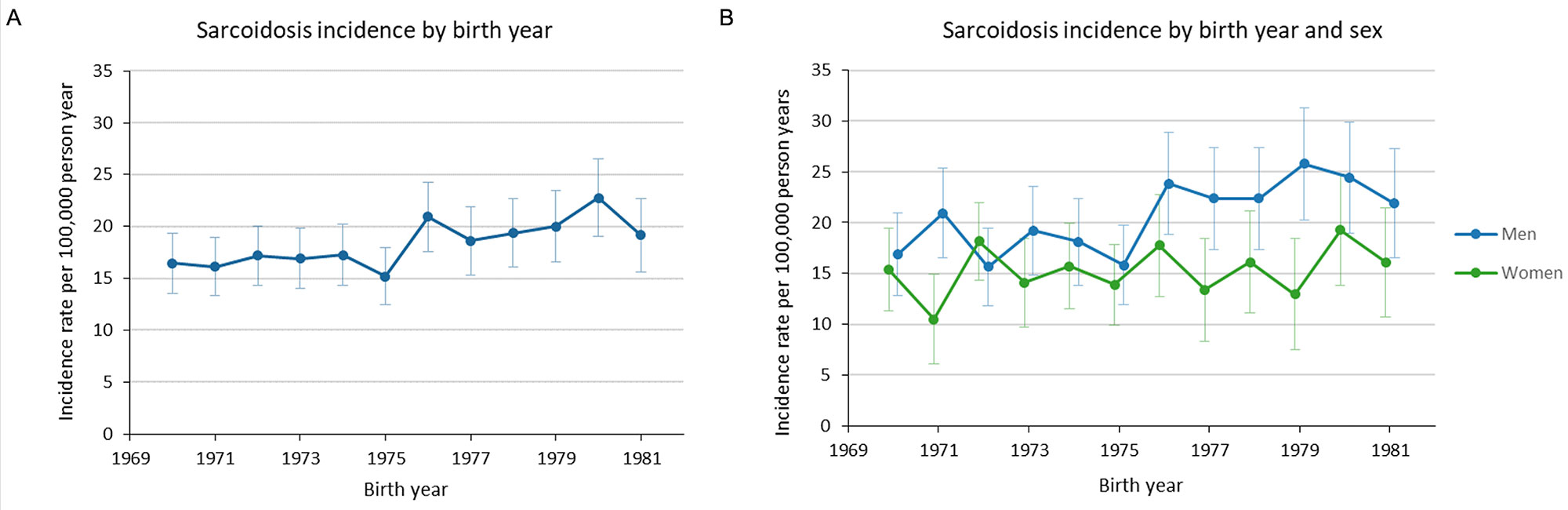
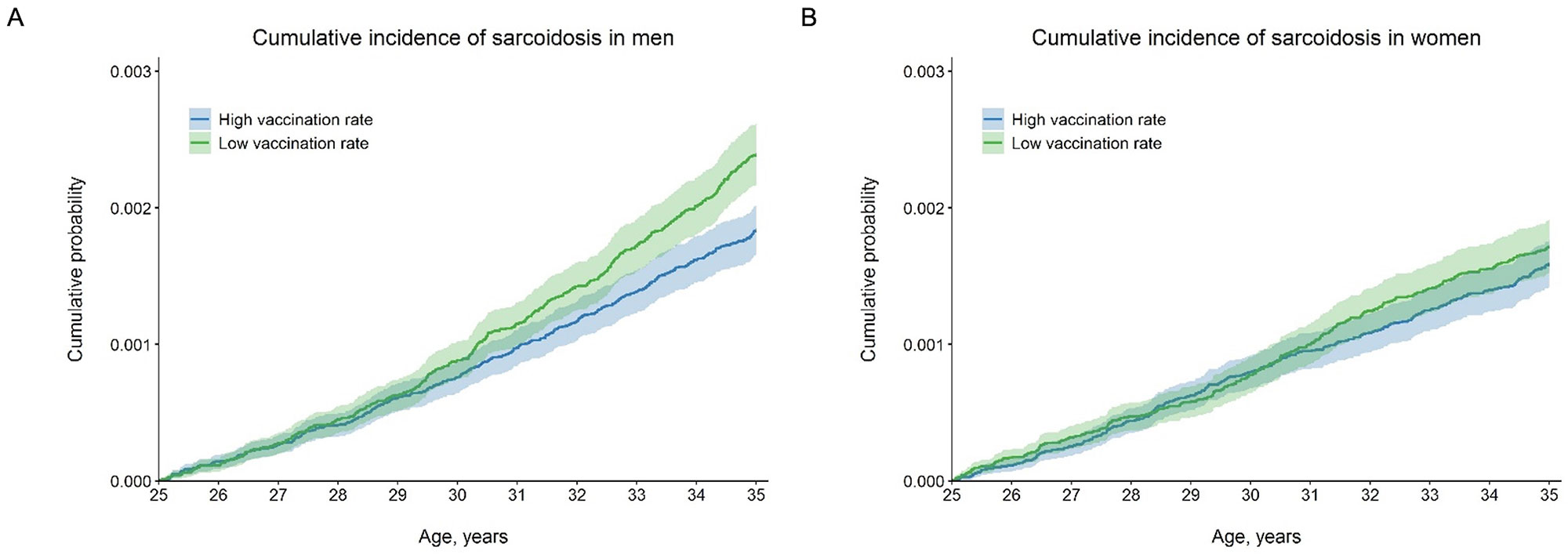
Results: Between 1995 and 2016 there were 11,199 incidence cases of sarcoidosis. The IR of sarcoidosis varied by year and sex, with an increase in cases in 2008 and a higher incidence among young males (Figure 1A and 1B). The IR of sarcoidosis was increased for those born in, or after, 1976 compared with those born before 1976 (the birth year corresponding to when BCG vaccination uptake precipitously declined) (Figure 2A). The increased incidence of sarcoidosis after 1976 was largely attributed to men (Figure 2B). The IRR for men in the years after BCG vaccination was stopped compared with men in the years before vaccination was stopped was 1.22 (95% confidence interval [CI] 1.02-1.45). In women, the IRR was 1.08 (95% CI 0.88-1.31, p=0.465). The cumulative incidence probability curves show an increased incidence of sarcoidosis in male patients born during low BCG vaccination use compared with male patients born during high BCG vaccination use (Figure 3A). This was not seen for female patients (Figure 3B).
Conclusion: Our study showed that BCG vaccination has an effect on the incidence rate of sarcoidosis in men, but not in women. The effect of BCG vaccination cannot be fully separated from the effect of calendar year, so the results must be interpreted with caution. However, these data support a potential protective effect of BCG vaccination, at least in men, against the development of sarcoidosis.
To cite this abstract in AMA style:
Baker M, Vágó E, Tamang S, Horváth-Puhó E, Sørensen H. Sarcoidosis Rates in BCG-Vaccinated and Unvaccinated Young Adults: A Danish Register-Based Study [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/sarcoidosis-rates-in-bcg-vaccinated-and-unvaccinated-young-adults-a-danish-register-based-study/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/sarcoidosis-rates-in-bcg-vaccinated-and-unvaccinated-young-adults-a-danish-register-based-study/