Session Information
Date: Saturday, November 6, 2021
Title: RA – Diagnosis, Manifestations, & Outcomes Poster I: Cardiovascular Pulmonary Disease (0268–0295)
Session Type: Poster Session A
Session Time: 8:30AM-10:30AM
Background/Purpose: Patients with rheumatoid arthritis (RA) are known to have an increased risk of developing, mainly ischemic cardiovascular diseases (CVD). This is partly explained by a higher incidence of traditional CV risk factors as hypertension and/or hypercholesterolemia but also due to the systemic inflammation characteristic to RA. RA is considered an independent CV risk by National and International CVD risk management guidelines, and therefore CVD risk screening is recommended. However, the implementation of CV risk management is often poorly performed in daily clinical practice.
The aim of the current study was to investigate the cardiovascular disease risk of newly diagnosed RA patients, and review if and to what extent implementation of CVD risk management had previously taken place.
Methods: Every newly diagnosed RA patient in a large Dutch outpatient rheumatology clinic had CV screening within their first year post-diagnosis during a regularly scheduled visit, where among others smoking habits, blood pressure and lipid profile were measured. A 10-year cardiovascular risk was calculated using a modified SCORE calculator from www.u-prevent.com, which predicts the risk of myocardial infarction, stroke, heart failure, peripheral arterial disease and CV death based on several CV risk factors. To account for RA as a risk factor, the calculator multiplies the risk by 1.5, in accordance with the Dutch CV risk management guideline. The calculated 10-year cardiovascular morbidity risk was categorized in low (< 10%), intermediate (10-19%) and high (≥20%), and the 10-year mortality risk was also categorized in low (< 1%), intermediate (1-4%) and high (≥5%).
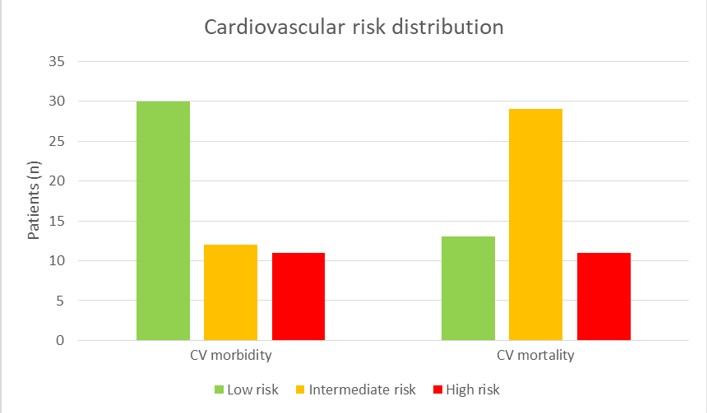
Results: A total of 53 patients were included up to this point. Of these, the average age was 57 (±8.5), and 39 (74%) were women. Mean systolic blood pressure was 129 (±17.7) mmHg, with 38 (72%) patients having hypertension. Mean total cholesterol, LDL and HDL were respectively 5.5 (±1.0) mmol, 3.43 (±0.82) mmol and 1.78 (±0.54) mmol, with 30 patients having hypercholesterolemia. The average calculated 10-year morbidity risk of all patients was 13%, and the mortality risk was 3%. Distribution of the 10-year risk in low, intermediate and high is presented in figure 1. Only one patient reported having previous used medication for hypercholesterolemia, but not at the time of enrollment in this study.
Conclusion: 43% of newly diagnosed RA patients had an intermediate or high calculated 10-year CV morbidity risk, and 76% had an intermediate or high mortality risk. Patients with early RA still often have underdiagnosed and severely undertreated risk factors of CVD, such as hypertension and hypercholesterolemia. Early CV risk assessment and management in patients with RA is critical and needs to be implemented as standard care.
To cite this abstract in AMA style:
Raadsen R, Hansildaar R, Heslinga M, van Kuijk A, Nurmohamed M. Risk of Cardiovascular Disease in Newly Diagnosed Rheumatoid Arthritis: A Current Risk Assessment [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/risk-of-cardiovascular-disease-in-newly-diagnosed-rheumatoid-arthritis-a-current-risk-assessment/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/risk-of-cardiovascular-disease-in-newly-diagnosed-rheumatoid-arthritis-a-current-risk-assessment/