Session Information
Date: Saturday, November 12, 2022
Title: Health Services Research Poster I: Lupus, RA, Spondyloarthritis and More
Session Type: Poster Session A
Session Time: 1:00PM-3:00PM
Background/Purpose: Low disease activity (LDA) is a key goal in treating Rheumatoid arthritis, but implementing the treat to target approach in clinical practice has been suboptimal (1). It would be desirable to survey disease activity status at the practice level. Traditionally, disease activity calculations are embedded in visit documentation, challenging data extraction and aggregation. The automated capture and storage of metrics to calculate major disease indices can generate practice population metrics. Barriers to treatment in high disease activity subjects can be specifically identified and targeted. This abstract reports on the process of implementing standardized metrics capture and reporting on a practice level.
Methods: Using the EPIC software system, the division of rheumatology adopted automated metrics capture of patient and provider global, swollen and tender joint counts, and acute phase reactants to calculate the clinical disease activity index (CDAI), disease activity score-28 ESR (DAS28-ESR), and DAS28-CRP. After one year, provider reports were concatenated, cleaned, extracted, and analyzed using the R-Studio software package. The CDAI metrics stratified subjects into high disease activity (HDA), moderate disease activity (MDA), and (LDA) or remission. A retrospective chart review evaluated factors contributing to high disease activity.
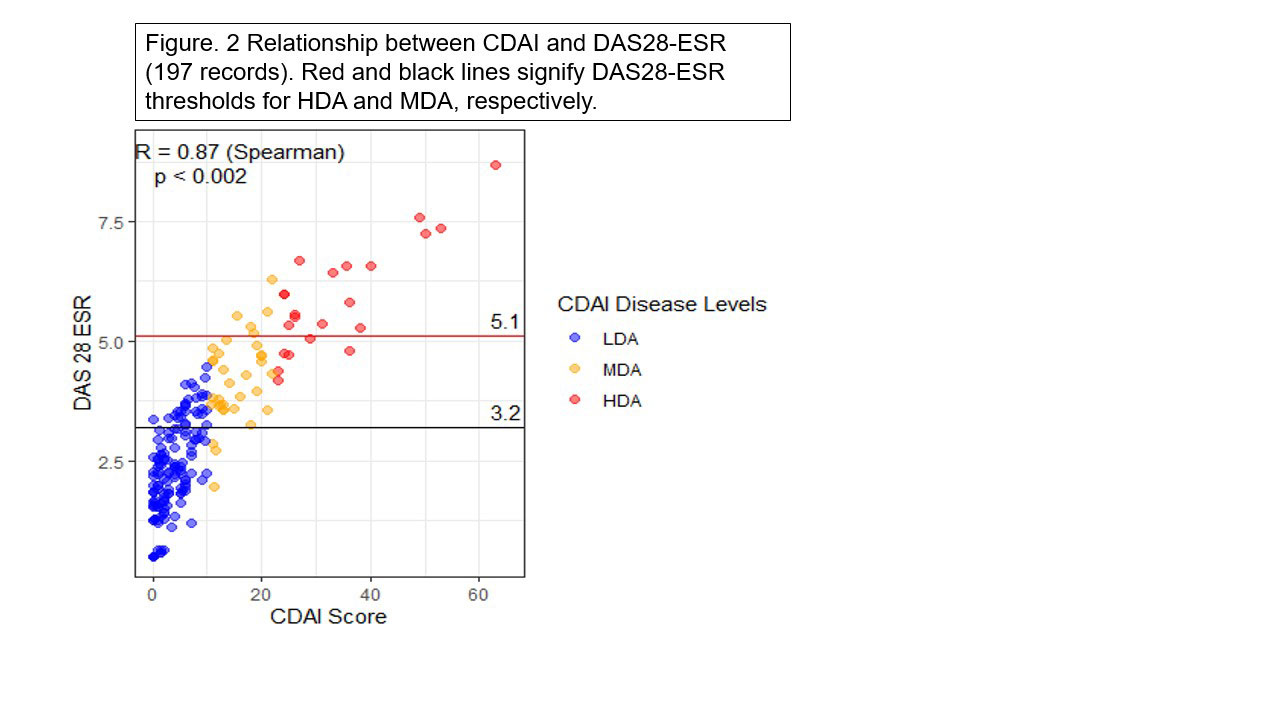
Results: Combining individual provider reports resulted in 3060 records. Elimination of duplicate cases, non-divisional providers, and non-rheumatoid arthritis patients resulted in 214 unique cases. CDAI was the most available metric, followed by DAS28-ESR. The mean age was 60.3 years, with no age differences across the disease strata. Of the population, 85% were female, 69% LDA, 17% MDA, 14% HDA. Fellows and a newer provider tended to see more severe subjects. (Fig 1). DAS28-ESR (197 records) classified more patients as MDA than CDAI. ( 31% vs.17% respectively). CDAI and DAS28-ESR had a good to excellent positive linear correlation (Figure 2) and agreement. (Weighted Kappa = 0.768). Subjects with high disease activity had several barriers to care. (Table 1). The most common reason was restricted access to modern disease modifying agents.
Conclusion: Automated capture and storage of disease activity metrics may enable snapshots of the disease activity of rheumatoid arthritis patients in clinical practice. High disease individuals can be identified for escalated interventions to overcome barriers to attaining control. The report of disease activity measures allows comparison across providers, including trainees, providing valuable insights into the acuity of subjects seen by individuals. The overall concordance of CDAI and DAS28-ESR is reassuring for making treatment decisions at the time of the office visit based on clinical metrics without waiting for the acute phase reactant results. Further enhancements would be to track individual subjects over time and automate the data handling to produce real-time practice dashboards.
References
1. Solomon DH, Losina E, et al. Implementation of Treat-to-Target in Rheumatoid Arthritis Through a Learning Collaborative: Results of a Randomized Controlled Trial. Arthritis & Rheumatology 2017;69:1374–1380.


To cite this abstract in AMA style:
Thway m, Kaeley G, Ramsubeik K, Ramrattan L, Otalora Rojas L, Singh S. Rheumatoid Arthritis – Are We Getting to Target? [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/rheumatoid-arthritis-are-we-getting-to-target/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/rheumatoid-arthritis-are-we-getting-to-target/