Session Information
Date: Sunday, November 7, 2021
Title: RA – Diagnosis, Manifestations, & Outcomes Poster II: Miscellaneous Aspects of RA (0786–0812)
Session Type: Poster Session B
Session Time: 8:30AM-10:30AM
Background/Purpose: The main goal of treatment for patients (pts.) with rheumatoid arthritis (RA) is to achieve remission, in order to both, preserve physical function and to stop and prevent radiographic progression. Using the treat-to-target (T2T) approach this has recently been achieved in less than 50% of pts. in an early arthritis cohort in Germany1. Several influencing factors such as long symptom duration, impaired physical function, and a history of multiple DMARD therapies were identified. Remission rates over longer periods of time in a real-life setting have not been well studied.
To evaluate the remission rate in a cohort of RA pts. treated in a tertiary care center in which a large proportion of pts. present for a second opinion.
Methods: Adult RA pts. were eligible for inclusion when their initial visit at our tertiary center was between January 2012 and December 2018. Patients and disease characteristics as well as standard assessments using validated outcome parameters for disease activity (DAS28-CRP, SDAI, and ACR/EULAR remission) and physical function (HAQ) were prospectively documented (clinical visit) and values were taken retrospectively from their initial visit (baseline visit) and from the visit at which remission criteria of DAS28-CRP < 2.6 occurred (remission visit).
Results: A total of 137 pts. were examined at their clinical visit between August 2020 and February 2021. Retrospective chart data were available for a follow-up of 33.7 (SD 18.0) months. One third of our cohort already had erosions and severe limitations in physical functioning (table 1). Cardiovascular comorbidities were as common as osteoporosis (both 13.1%). The vast majority of pts. (110 (80.3%)) achieved a state of clinical remission, (DAS28-CRP < 2.6) at least once in a time period of 47.9 (SD 18.9) months. At the clinical visit, 41 pts. (29.9%) were in DAS28 remission. However, using other outcome measures, 23 pts. achieved remission using SDAI (16.8%) and only 17 with Boolean criteria (12.4%), respectively. On average, remission by DAS28-CRP was reached 14.9 (SD 13.8) months after baseline visit. During the observation period pts. achieved remission for 15.8 (SD 10.4) months or 51.3% (SD 25.7) of the time, while 65 pts. (47.4%) achieved sustained remission for at least 6 months. Pts. with comorbidities reached remission less often than pts. without comorbidity (p=0.002). In accordance with the T2T strategy and EULAR recommendations, glucocorticoids were stopped in 47 pts. (34.3%) during the observation period. The remaining 53 pts. (38.7%) were still taking glucocorticoids at the clinical visit, but at a significantly lower dose than at baseline (table 2). The number of pts. on b/ts-DMARD therapy increased significantly from 14.7% at baseline to 59.1% at the clinical visit.
Conclusion: In this study pts. with RA reached remission more often when visited and observed more frequently and for longer periods of time. However, disease activity tends to come back for different reasons. This needs to be further investigated. Moreover, the data also indicate that in a chronic disease more long term data are needed since short term results may show efficacy but this frequently changes over time in both directions.
Reference:1 Albrecht Z Rheumatol 2021
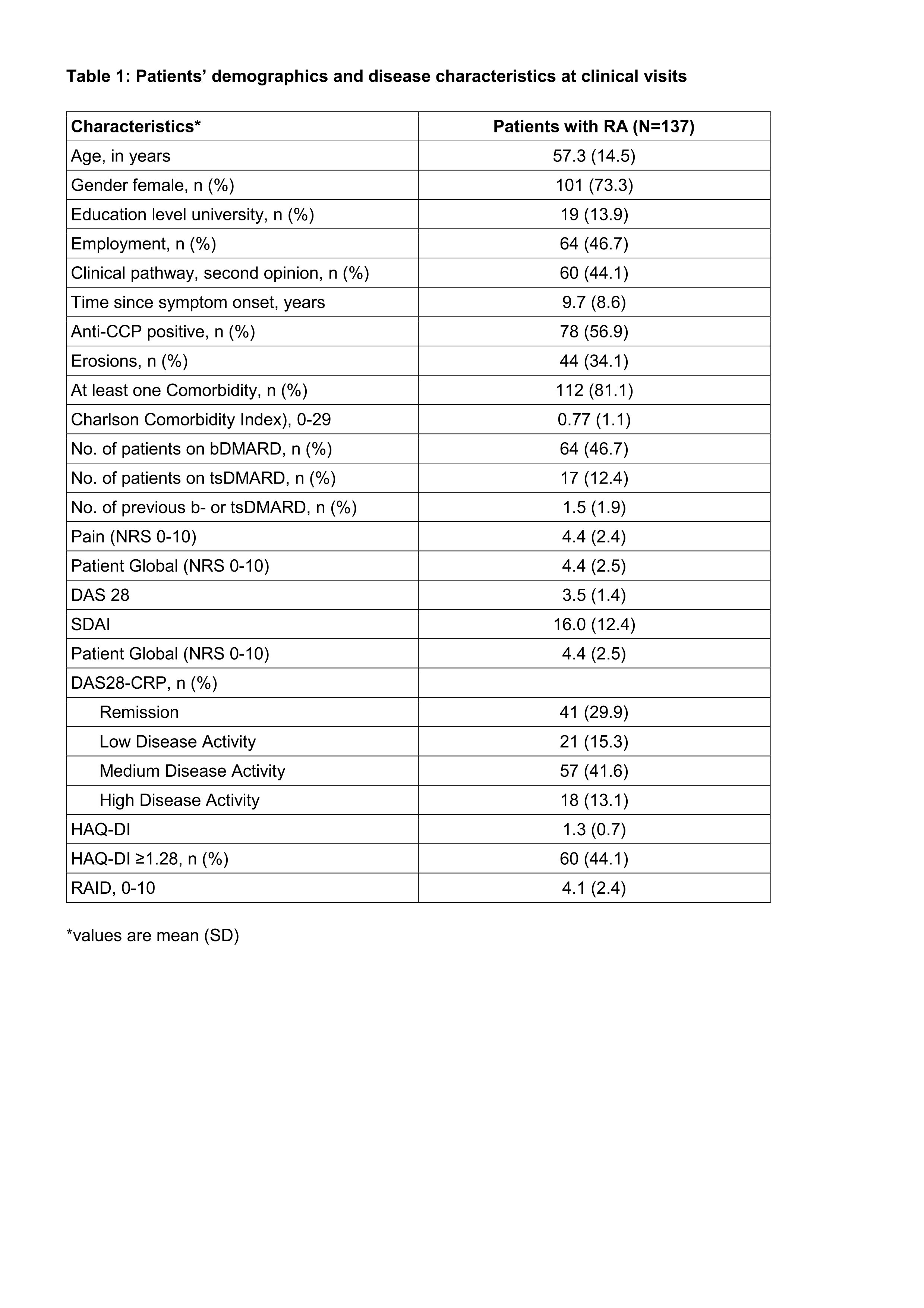
Table legend on the bottom: *values are mean (SD)
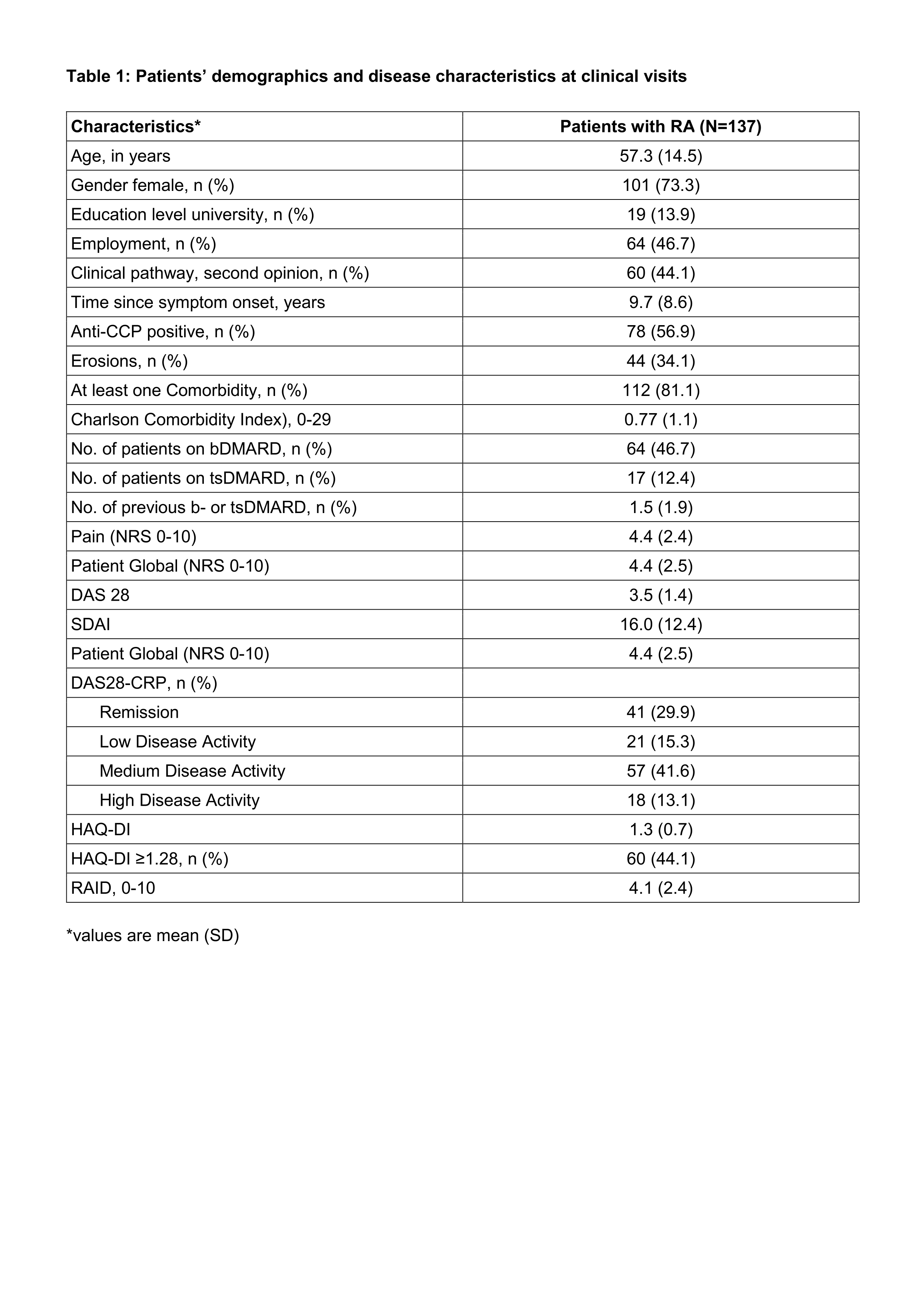
Table legend on the bottom: *values are mean (SD)

To cite this abstract in AMA style:
Gildemeister N, Redeker I, Buehring B, Andreica I, Kiefer D, Baraliakos X, Braun J, Kiltz U. Remission Rates of Patients with Rheumatoid Arthritis in a Tertiary Care [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/remission-rates-of-patients-with-rheumatoid-arthritis-in-a-tertiary-care/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/remission-rates-of-patients-with-rheumatoid-arthritis-in-a-tertiary-care/