Session Information
Date: Friday, November 6, 2020
Title: Patient Outcomes, Preferences, & Attitudes Poster I: RA, Spondyloarthritis, & OA
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: We previously showed rheumatoid arthritis (RA) patients report diversity in disease activity (DA) patterns that may be associated with treatment response. Patients who describe their DA as a flaring or non-progressing pattern are more likely to experience high levels of DA improvement (≥70%). We aimed to better understand the relationship between RA disease activity patterns and rheumatology treatment experiences.
Methods: An anonymous 28-item questionnaire was developed and pilot-tested by the study team and presented in 2019 on a secure online survey system. Eligible participants were U.S. residents age ≥18 years with a self-reported medical diagnosis of RA. They were asked questions about socio-demographics, RA disease activity, diagnosis and DMARD history, improvement from RA treatment, and RA treatment goals created with their provider. Further, patients were asked which of a list of disease patterns best described their DA (see figure 1). The patterns were divided into 2 categories: constant vs flaring and remitting and progressive vs non-progressing.
Results: 907 people responded (90% women, 10% men), with a mean age of 58 years and 11.1 years since diagnosis (SD 10.1). Of the 886 people who responded to the disease pattern questions, 46% had constant and 54% were flaring/remitting. Similarly, 60% were progressive and 40% were non-progressing. Longer times from symptom onset to RA diagnosis associated with constant DA patterns (< 6mo 38%, >6mo to < 5yr 46%, >5yr 52%) and progressive DA patterns (< 6mo 50%, >6mo to < 5yr 60%, >5yr 70%).
Moderate-severe levels of DA were more common with constant and progressive patterns (constant 94%, flaring 59%, progressive 88%, non-progressing 54%). Those with constant disease were less likely to say they were in remission (constant 0%, flaring 6%) or have had their doctor say they were in remission (2% and 15%, respectively). Those with progressive disease gave similar responses for being in RA remission (progressive 1%, non-progressing 6%) or diagnosis of remission (6% and 14%, respectively). Those with constant or progressive DA were more likely to say they were in a poor/very poor state of health (constant 33%, flaring 12%, progressive 28%, non-progressing 14%).
Fewer people with constant or progressive disease were satisfied/very satisfied with their rheumatology treatment (constant 63%, flaring 79%, progressive 67%, non-progressing 76%). People with progressive disease were less likely to be asked by their providers about RA treatment goals (progressive 33%, non-progressive 42%). Respondents strongly supported the use of materials to enhance treatment goal discussions with their rheumatology providers.
Conclusion: This survey found previously unreported associations between patterns of RA disease activity and interfaces with rheumatology care including time to initiation of RA treatment, satisfaction with rheumatology care, and occurrence of shared treatment goal discussions as well as higher levels of DA and fewer remissions of disease. Further research should seek greater understanding of the significance of DA patterns in RA treatment and whether patients with more aggressive DA patterns should have adapted treatment recommendations.
 Fig.1 Patterns of RA Disease Activity
Fig.1 Patterns of RA Disease Activity
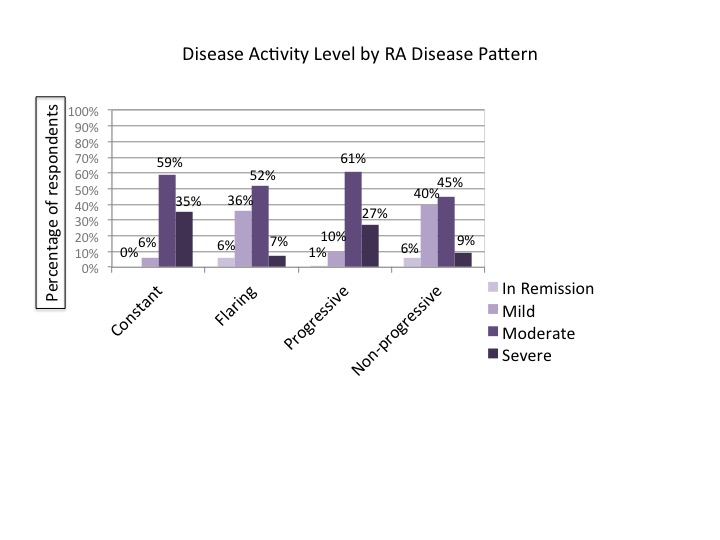 Fig.2 Disease Activity Level by RA Disease Pattern
Fig.2 Disease Activity Level by RA Disease Pattern
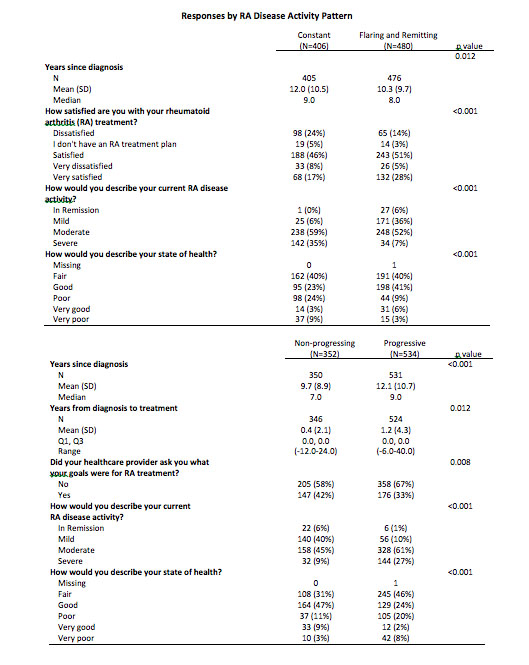 Table1 Responses by RA Disease Activity Pattern
Table1 Responses by RA Disease Activity Pattern
To cite this abstract in AMA style:
O'Neill K, Marks K, Davis J, Crowson C. Relationships Between Disease Patterns in RA and Rheumatology Treatment [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/relationships-between-disease-patterns-in-ra-and-rheumatology-treatment/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/relationships-between-disease-patterns-in-ra-and-rheumatology-treatment/