Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Systemic sclerosis (SSc) is a chronic autoimmune disease known for its fibrotic and vascular complications impacting various organs, including the heart. Myocardial involvement causes significant morbidity and mortality in SSc patients. Early detection of myocardial involvement is challenging as patients often remain asymptomatic until they progress. Traditional transthoracic echocardiogram (TTE), the currently accepted periodic screening tool for ventricular dysfunction and pulmonary hypertension, may not capture early/subclinical myocardial dysfunction. Strain echocardiography, an emerging technique that measures myocardial length during all phases of the cardiac cycle, is an inexpensive tool that measures myocardial deformation and shows promise in assessing cardiac health in SSc patients. However, limited research exists on the temporal progression of strain in this population and its correlation with the traditional TTE. Our study aimed to evaluate the evolution of left ventricular global longitudinal strain (GLS) and to demonstrate its role in early detection of left ventricular dysfunction (LVD), even when TTE is reported normal.
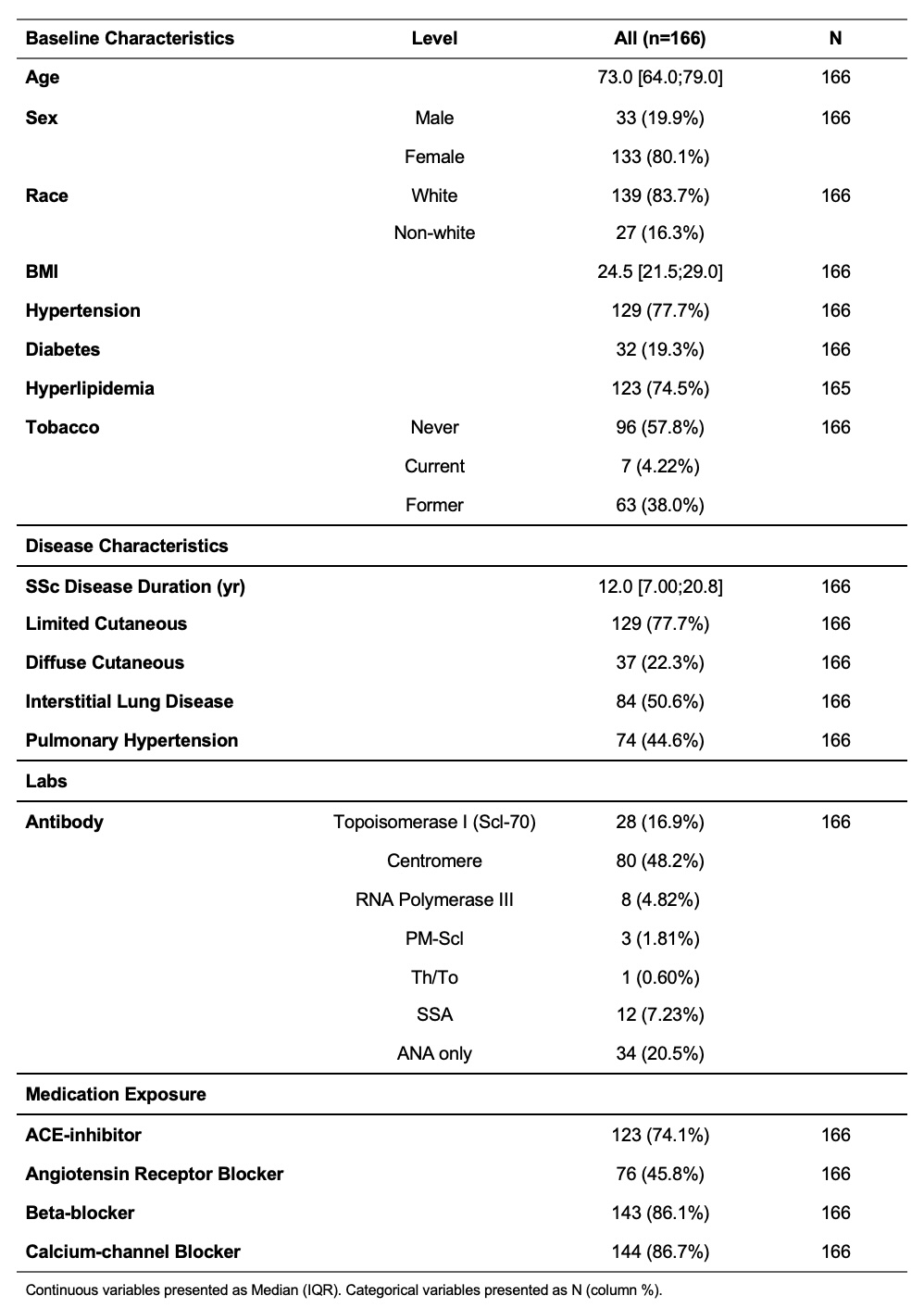
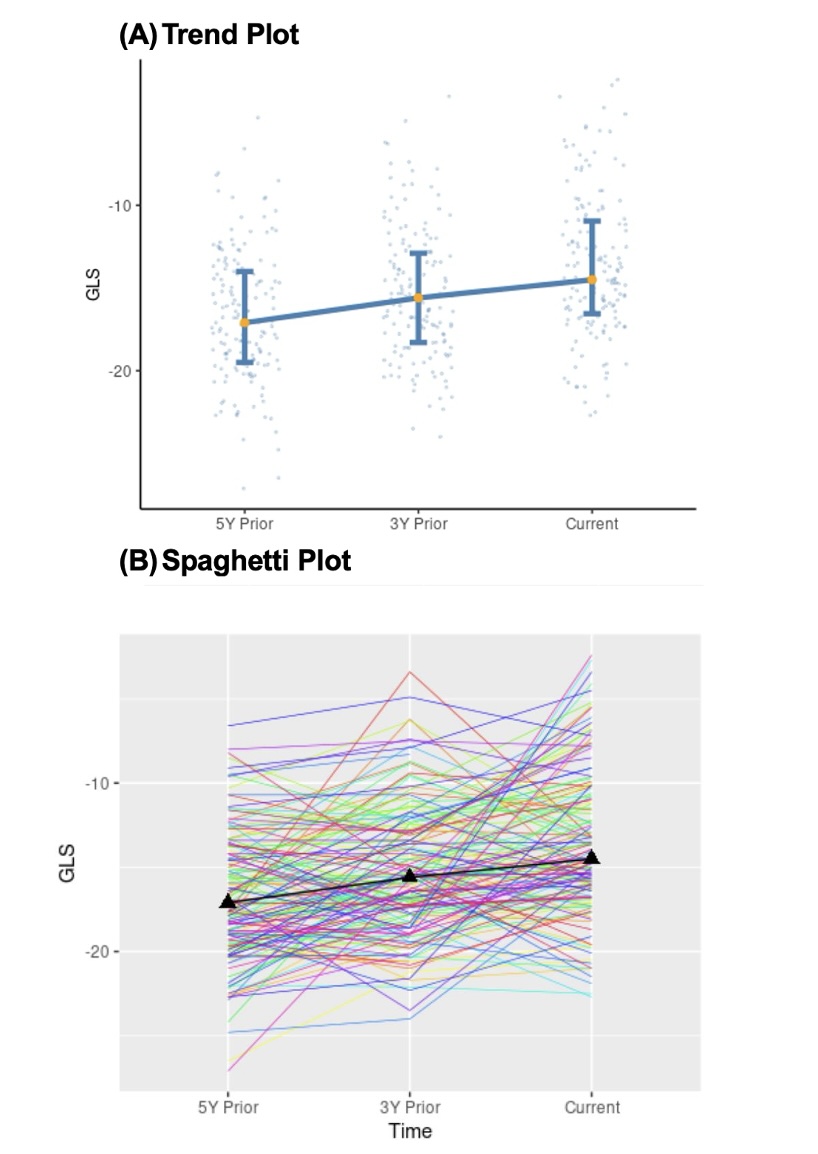
Methods: We conducted a retrospective analysis on SSc patients (2013 ACR criteria, Table 1) currently diagnosed with LV diastolic and/or systolic dysfunction (LVD) who had undergone at least 3 TTEs over the past decade. GLS values were obtained using speckle-tracking echocardiography from the most recent TTE and those from 3 and 5 years prior. To ensure consistency, we recalculated all GLS values using TomTec® technology. The GLS trend was plotted (Fig. 1). A generalized estimating equation (GEE) modeled the relationship between GLS and LVD, incorporating repeated measurements with an exchangeable correlation structure. Adjustments were made for known heart failure risk factors (age, gender, hypertension, hyperlipidemia, diabetes, disease duration, pulmonary hypertension, and tobacco use).
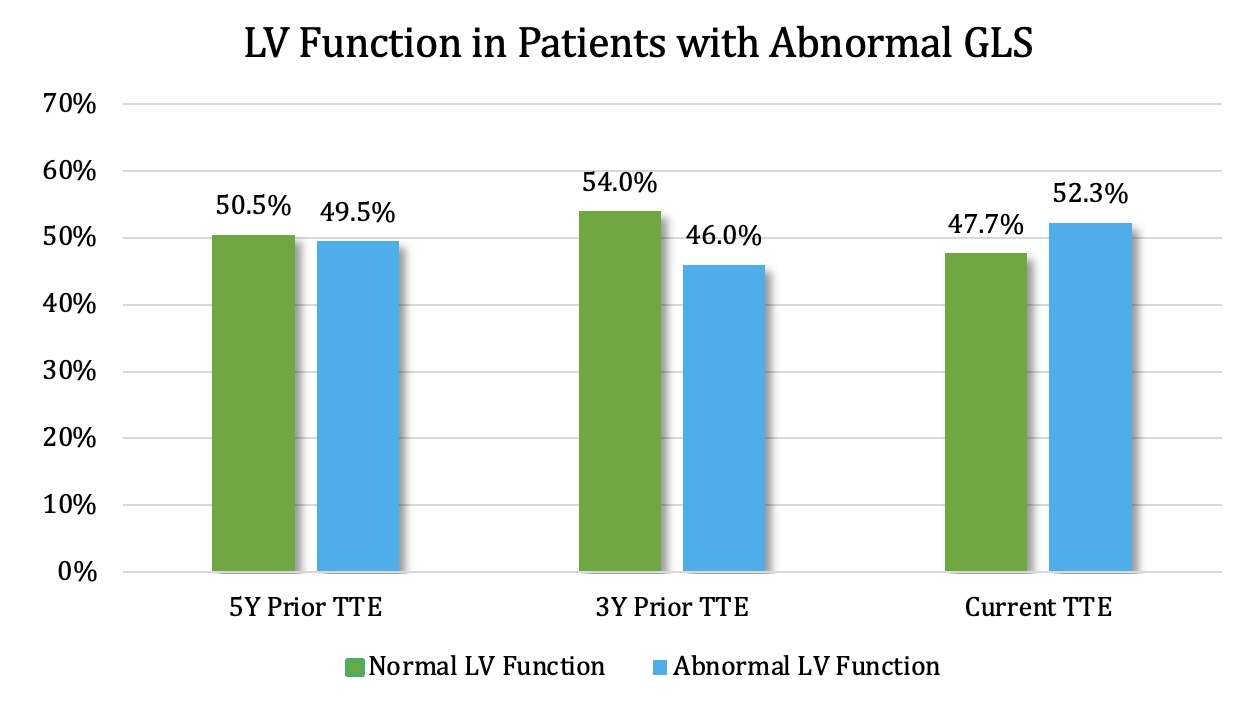
Results: GLS is expressed as a negative percentage [normal > -18%; abnormal ≤ -18%]. There was a progressive decline in GLS values: -17.1% 5 years prior → -15.6% 3 years prior → current strain of -14.5%. A less negative GLS value, older age, and being a non-diabetic were associated with LVD. Half of the patients (51%) with normal LV function on TTE (LVEF ≥ 50% and normal diastolic function) 5 years prior exhibited abnormal GLS values at that time. This discrepancy persisted over time, indicating that, in general, in SSc patients with heart failure, GLS captures LVD in twice as many patients as their TTE. Though we only included patients with SSc-LVD in our study, 47.7% did not show LVD on their current TTE (Fig. 2), perhaps because in this retrospective analysis, we could not accurately account for the treatment-related normalization of the current LVD in some patients (detected by conventional TTE).
Conclusion: Our research highlights the importance of GLS in detecting LVD in SSc patients. Interestingly, around half of the patients with normal LV function at all time points had an abnormal GLS. Therefore, incorporating GLS into routine screening may help identify LVD in more SSc patients, leading to early intervention and potentially improving patient outcomes and survival.
To cite this abstract in AMA style:
Abdalla J, Okushi Y, Zhang C, Popovic Z, Wassif H, Chatterjee S. Progression of Global Longitudinal Strain and Identification of Left Ventricular Dysfunction in Systemic Sclerosis Patients [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/progression-of-global-longitudinal-strain-and-identification-of-left-ventricular-dysfunction-in-systemic-sclerosis-patients/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/progression-of-global-longitudinal-strain-and-identification-of-left-ventricular-dysfunction-in-systemic-sclerosis-patients/