Session Information
Date: Sunday, October 26, 2025
Title: (0671–0710) Systemic Sclerosis & Related Disorders – Clinical Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Scleroderma Renal Crisis (SRC) is a severe manifestation of Systemic Sclerosis (SSc) associated with elevated morbidity and mortality. We aimed to address the challenges of studying this rare condition by collecting and analyzing data to further our understanding of SRC. This research builds upon our previous work presented at ACR in 2022. We previously found that patients who did not have a diagnosis of SSc before SRC had a statistically significant higher odds of requiring hemodialysis (HD) during SRC compared to patients who had a prior diagnosis of SSc. We also found that patients with a history of hypertension (HTN) had a statistically significant higher odds of 1-year mortality compared to patients without HTN. We did not find any statistically significant increase in the odds of severe outcomes in SRC for African-American patients, patients with RNA Polymerase III antibodies, or patients with late SRC.
Methods: We obtained data through chart review of 44 patients at our institution who developed SRC between 2008 and 2020. All patients met ACR/EULAR 2013 classification criteria for SSc. We evaluated predictors of HD at time of SRC and 1-year mortality post-SRC using Fisher’s exact tests and Wilcoxon rank-sum tests, and we reported related p-values.
Results: Table 1 includes selected characteristics of our patients with SRC. We found that patients who required HD at time of SRC had a statistically significant elevation in creatinine and decreases in platelet count and hemoglobin, compared to patients who did not require HD (Table 2). While there were no statistically significant differences regarding HD need at time of SRC based on sex, specialist care, or presence of schistocytes on peripheral blood smear (PBS), there were trends toward statistical significance. Furthermore, we found statistically significant differences in 1-year mortality based on patient sex and age (Table 3). Male sex and older age were associated with 1-year mortality, which supports previously reported findings (1). There was not a statistically significant difference in 1-year mortality between patients on HD 6 months-post SRC and those who were not on HD 6 months-post SRC.
Conclusion: We identified statistically and clinically significant differences in SRC lab parameters between patients who required HD at SRC and those who did not. The median creatinine and hemoglobin levels differed by over one unit, and thrombocytopenia was a predictor of HD requirement at SRC. Because there were trends toward statistical significance for sex, specialist care, and presence of schistocytes regarding HD requirement, we hope to reevaluate these potential predictors on larger datasets. We found that older age and male sex were associated with elevated 1-year mortality. Combining these results with our previous findings, we have identified several predictors of severe outcomes in SRC. These findings can assist clinicians with risk-stratification of SRC patients, lay the groundwork for future research, and help mitigate severe outcomes.1. Steen VD, Medsger TA Jr. Long-term outcomes of scleroderma renal crisis. Ann Intern Med. 2000 Oct 17;133(8):600-3. doi: 10.7326/0003-4819-133-8-200010170-00010. PMID: 11033587.
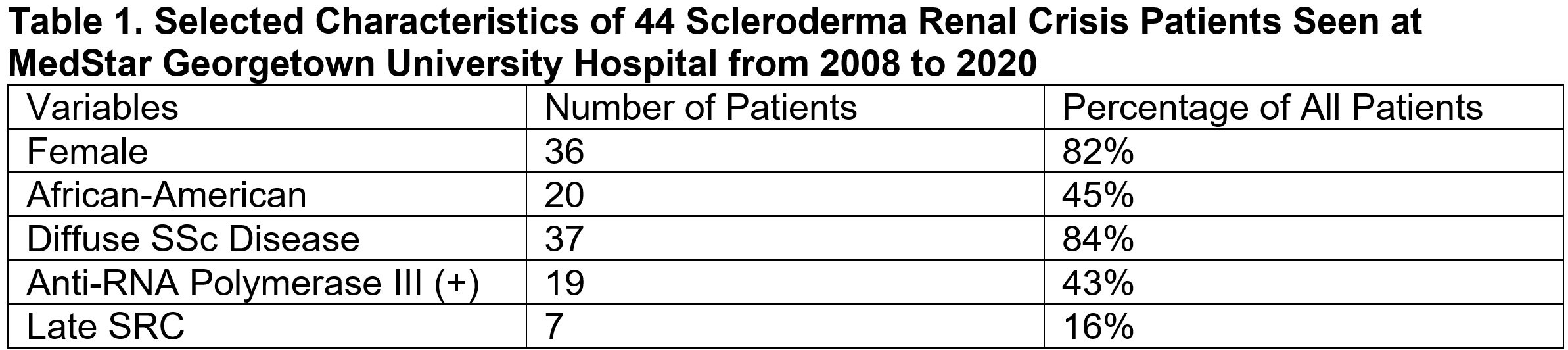 Legend: SSc = Systemic Sclerosis, also known as Scleroderma, Anti-RNA Polymerase III (+) = Patients
Legend: SSc = Systemic Sclerosis, also known as Scleroderma, Anti-RNA Polymerase III (+) = Patients
who tested positive for the Anti-RNA Polymerase III antibody, SRC = Scleroderma Renal Crisis,
Late SRC = Patients with at least 4 years between first SSc symptom and SRC. The mean age of
patients was 51.5, and the ages of patients ranged from 27 to 88 years old.
.jpg) Legend: SRC = Scleroderma Renal Crisis, HD = Hemodialysis, Dx = Diagnosis, Specialist Care = Patients
Legend: SRC = Scleroderma Renal Crisis, HD = Hemodialysis, Dx = Diagnosis, Specialist Care = Patients
under the care of a rheumatologist with Scleroderma expertise, Schistocytes = Presence of schistocytes
on a peripheral blood smear at the time of Scleroderma Renal Crisis diagnosis. For continuous variables,
median and interquartile range (Q1 and Q3) are reported. For categorical variables, proportions (%) are
reported. Statistically significant P-values are bolded. *One patient had missing data regarding dialysis
need at Scleroderma Renal Crisis Presentation.
.jpg) Legend: SRC = Scleroderma Renal Crisis, HD = Hemodialysis. For continuous variables,
Legend: SRC = Scleroderma Renal Crisis, HD = Hemodialysis. For continuous variables,
median and interquartile range (Q1 and Q3) are reported. For categorical variables,
proportions (%) are reported. Statistically significant P-values are bolded. *One patient had
missing data regarding 1-year mortality after Scleroderma Renal Crisis.
To cite this abstract in AMA style:
Luta A, Mitchell S, Steen V. Predictors of Severe Outcomes in Scleroderma Renal Crisis: Updated Results from a Single Center Study [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/predictors-of-severe-outcomes-in-scleroderma-renal-crisis-updated-results-from-a-single-center-study/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/predictors-of-severe-outcomes-in-scleroderma-renal-crisis-updated-results-from-a-single-center-study/