Session Information
Date: Sunday, October 26, 2025
Title: (0210–0232) Measures & Measurement of Healthcare Quality Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Comorbid anxiety (ANX), depression (DEP), and fibromyalgia(FM) are reported as more common in patients with rheumatoid arthritis (RA) and other rheumatic diagnoses than in the general population. These comorbidities are associated with elevated RA indices such as DAS28 and CDAI designed to assess inflammatory activity. However, formal recognition of ANX, DEP, and/or FM is largely limited to research studies, as multiple patient questionnaires are not feasible in busy routine care. Three validated indices within a multidimensional health assessment questionnaire (MDHAQ), MAS 2 – MDHAQ anxiety screen, MDS2 – MDHAQ depression screen, and FAST4 – fibromyalgia assessment screening tool, agree >80% with reference questionnaires. We analyzed the prevalence of positive MDHAQ screening for comorbid ANX, DEP, and/or FM on MDHAQ indices in unselected routine care patients with any rheumatic diagnosis seen at an academic medical center.
Methods: All patients with all diagnoses at the study site are asked to complete an MDHAQ at each rheumatology visit prior to seeing a health professional. The prevalence of positive screening on the MDHAQ indices for ANX, DEP, and FM was computed according to ICD-10 diagnoses. Diagnoses with fewer than 20 patients were grouped as “other inflammatory” (other inflam) or “other noninflammatory” (other non-inflam).
Results: In 1337 patients, excluding 60 with primary FM, positive screening for MAS2 ANX, MDS2 DEP and/or FAST4 FM was seen in 587 (44%), including 399 (30%) for MAS2 ANX, 321 (24%) for MDS2 DEP, 328 (25%) for FAST4 FM; 750 patients (56%) screened negative for all the 3 indices (Table). Among diagnosis categories, a positive screen for any of the 3 indices ranged from 52% in patients with “other non-inflammatory” diagnoses, excluding primary fibromyalgia, to 30% in crystal diseases and vasculitis, for ANX from 39% in “other non-inflammatory” diagnoses to 19% in “other-inflammatory” diagnoses, for DEP from 33% in myositis to 9% in systemic sclerosis to, and for FM from 31% in OA to 7% in vasculitis (Table). The totals were raised by only 1% with inclusion of 60 patients with primary FM, reflecting a high prevalence of 1 , 2, or 3 positive screens in all other diagnosis categories (Table). Among all patients with a positive MDHAQ screening index for ANX, DEP, and/or FM, one of the 3 was positive in 271 (43%), 2 of the 3 in 214 (34%), and all 3 in 149 (24%) (Figure).
Conclusion: In 1337 patients seen in routine care (excluding 60 with primary FM), positive screening on MDHAQ indices was seen in 30% for ANX, 24% for DEP, 25% for FM, and 44% for any of the 3 indices. Positive screening is common, and affects assessment, management, and outcomes of all rheumatic diseases,. An important limitation involves data from only one setting, as variation is likely according to cultural and socioeconomic variables in different settings. An MDHAQ, completed by most patients in 5-10 minutes prior to seeing a rheumatologist and available in the February 2025 release of the Epic electronic medical record (EMR), provides a feasible strategy to screen for ANX, DEP, and FM in all patients.
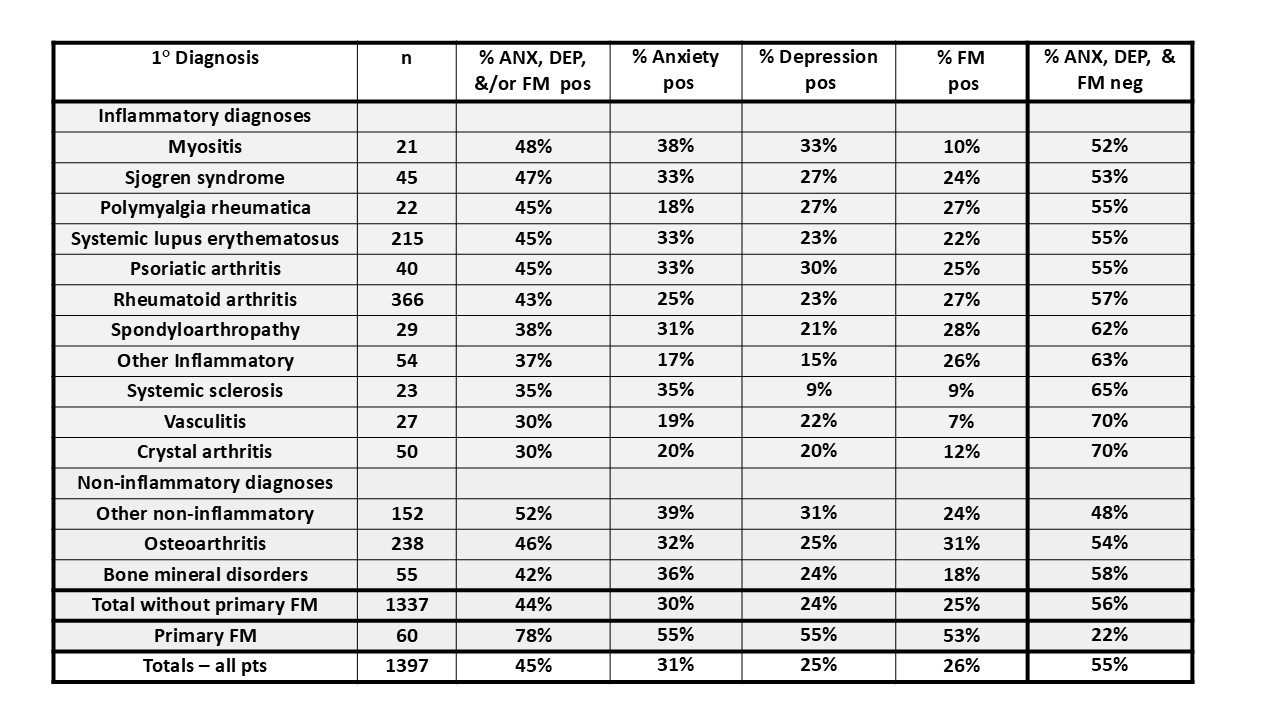 Table: Proportion of patients in each category who screen positive or negative for any of the
Table: Proportion of patients in each category who screen positive or negative for any of the
3 MDHAQ indices for anxiety, depression, and/or fibromyalgia and each individual index
.jpg) Figure: positive screening for anxiety, depression and fibromyalgia in rheumatology patients with all diagnoses seen in routine rheumatology care.
Figure: positive screening for anxiety, depression and fibromyalgia in rheumatology patients with all diagnoses seen in routine rheumatology care.
To cite this abstract in AMA style:
Schmukler J, Li T, Pincus T. Positive anxiety, depression and/or fibromyalgia screening on validated MDHAQ indices is seen in 30-50% of routine care patients with all rheumatic diagnoses [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/positive-anxiety-depression-and-or-fibromyalgia-screening-on-validated-mdhaq-indices-is-seen-in-30-50-of-routine-care-patients-with-all-rheumatic-diagnoses/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/positive-anxiety-depression-and-or-fibromyalgia-screening-on-validated-mdhaq-indices-is-seen-in-30-50-of-routine-care-patients-with-all-rheumatic-diagnoses/