Session Information
Date: Monday, November 9, 2020
Title: Pediatric Rheumatology – Clinical Poster III: SLE, Vasculitis, & JDM
Session Type: Poster Session D
Session Time: 9:00AM-11:00AM
Background/Purpose: Childhood-onset Takayasu Arteritis (c-TA) is a rare, granulomatous, chronic large-vessel vasculitis that involves mostly the aorta and its major branches with a high mortality rate (~35%) related to cardiovascular diseases, such as arterial occlusions and stenosis, ischemia or aneurysm formations. Due to the putative limitations imposed by the disease, the cardiovascular involvement, and other indirect factors (e.g., superprotection by parents and health practitioners, low self-efficacy and, social isolation), one could speculate that c-TA patients could also experience low physical activity levels and decreased aerobic conditioning. Therefore, assessing physical activity and cardiorespiratory fitness levels along with health-related quality of life (HRQL) and various traditional and non-traditional risk factors related to physical activity and physical capacity among c-TA patients vs. healthy controls remains clinically relevant for clinical practitioners.
Methods: We recruited c-TA patients with non-active disease (n=17) from three rheumatological centers in Sao Paulo. An age- and sex-matched healthy controls (n=17) were also enrolled in the study. We assessed physical activity levels (Actigraph GT3X accelerometers), aerobic capacity (a maximum graded exercise test on a treadmill), systemic inflammation (IFN-γ, IL-10, IL-12p70, IL-1ra, IL-1β, IL-6, TNF-α, VEGF and PDGF), cardiometabolic markers, disease-related parameters (Indian Takayasu Arteritis Clinical Activity Score; ITAS2010 and Pediatric Vasculitis Activity Score; PVAS), and HRQL (short-form health survey with 36 questions).
Results: The summary results from this study can be found in Figure 1. c-TA patients showed greater time spent in sedentary behavior (P=0.010), and lower moderate-to-vigorous physical activity (P>0.001) and lower step counts per day (P>0.001). VO2rpc (P< 0.001), VO2peak (P< 0.001) and chronotropic response (P=0.016) were significantly lower in c-TA patients. c-TA patients had worse HRQL in physical domain (P< 0.001). In the SF-36 subscales, functional capacity, physical appearance, and general health status were reduced in patients in comparison with CTRL (all P< 0.05). Inflammatory and angiogenesis markers did not differ between groups. However, c-TA patients displayed worse insulin sensitivity, based on insulin fasting (P=0.050), HOMA-IR (P=0.033) and lower HDL cholesterol levels (P=0.017) vs. CTRL (data not shown).
Conclusion: c-TA patients exhibited reduced physical activity levels and aerobic capacity, worse cardiometabolic risk factors and HRQL parameter compared with healthy peers. Physical inactivity and aerobic deconditioning emerge as potentially novel risk factors for c-TA. The role of physical activity interventions in preventing poor outcomes and improving HRQL in c-TA remains to be explored.
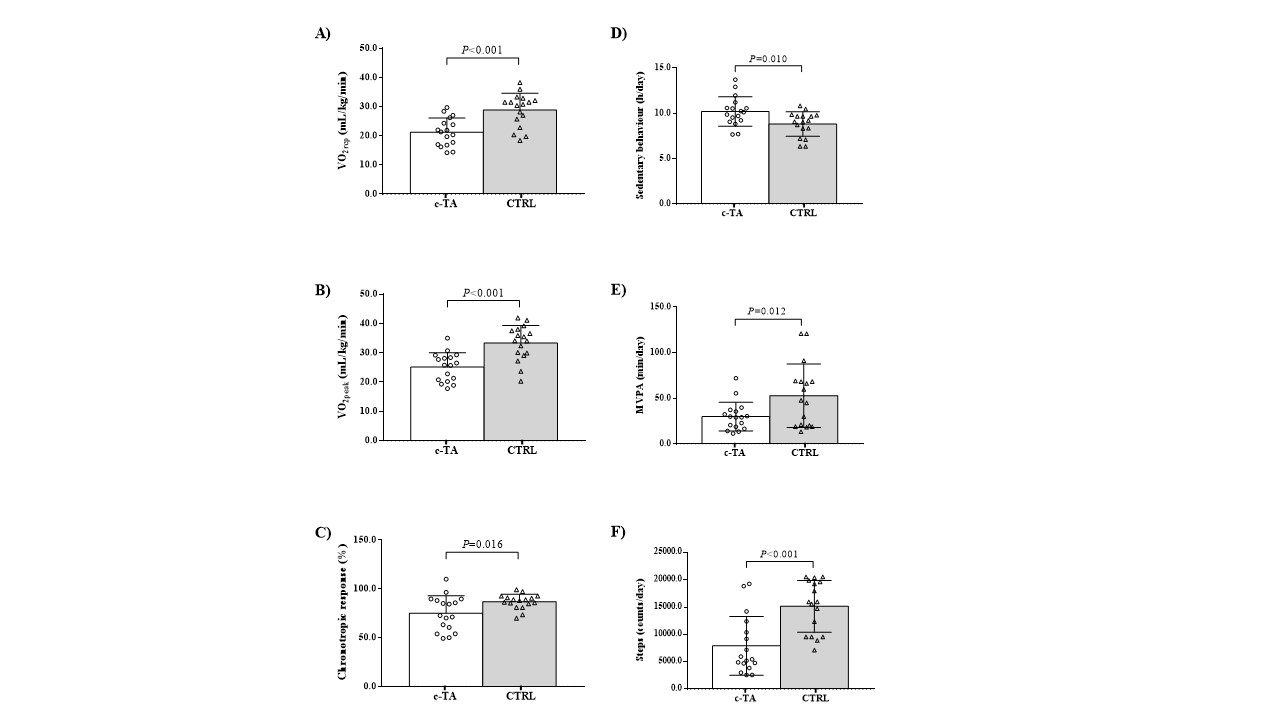 Cardiorespiratory fitness and objectively-measured physical activity in patients with childhood-onset Takayasu Arteritis (c-TA) and healthy controls (CTRL). Panel A) Respiratory compensation point (VO2rcp); Panel B) Peak oxygen uptake (VO2peak); Panel C) chronotropic response; Panel D) Sedentary behavior; Panel E) Moderate-to-vigorous physical activity (MVPA); Panel F) Steps per day.
Cardiorespiratory fitness and objectively-measured physical activity in patients with childhood-onset Takayasu Arteritis (c-TA) and healthy controls (CTRL). Panel A) Respiratory compensation point (VO2rcp); Panel B) Peak oxygen uptake (VO2peak); Panel C) chronotropic response; Panel D) Sedentary behavior; Panel E) Moderate-to-vigorous physical activity (MVPA); Panel F) Steps per day.
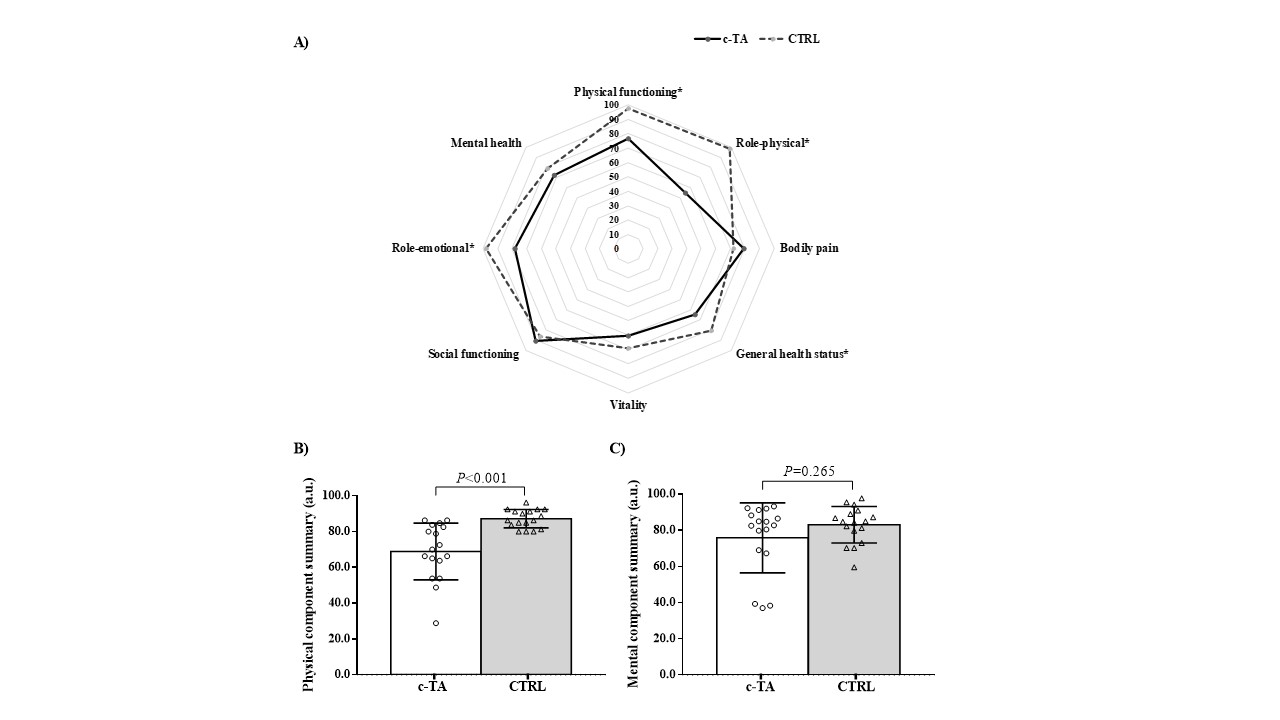 Healthy-related quality of life in patients with childhood-onset Takayasu Arteritis (c-TA) and healthy controls (CTRL). Panel A) Short Form-36 health survey domains between-group; B) Physical health domain; Panel C) Mental health domain.
Healthy-related quality of life in patients with childhood-onset Takayasu Arteritis (c-TA) and healthy controls (CTRL). Panel A) Short Form-36 health survey domains between-group; B) Physical health domain; Panel C) Mental health domain.
To cite this abstract in AMA style:
Astley C, Gil S, Clemente G, Terreri M, Campos L, Aikawa N, de-Sá Pinto A, Pereira R, Roschel H, Gualano B. Poor Physical Activity Levels and Cardiorespiratory Fitness Among Patients with Childhood-Onset Takayasu Arteritis in Remission [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/poor-physical-activity-levels-and-cardiorespiratory-fitness-among-patients-with-childhood-onset-takayasu-arteritis-in-remission/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/poor-physical-activity-levels-and-cardiorespiratory-fitness-among-patients-with-childhood-onset-takayasu-arteritis-in-remission/