Session Information
Date: Monday, November 9, 2020
Session Type: Poster Session D
Session Time: 9:00AM-11:00AM
Background/Purpose: Joint pain is a common presenting complaint in Primary Care with around 54.4 million adults diagnosed with some form of arthritis per 2013 CDC survey. Polyarthritis is defined as joint symptoms involving >/= 5 joints. It includes inflammatory and non-inflammatory arthritis. Rheumatoid arthritis (RA) is a primary consideration of inflammatory polyarthritis. Per the current American College of Rheumatology (ACR) classification criteria, the work up of inflammatory polyarthritis should include CBC, ESR, Rheumatoid Factor (RF), anti-cyclic citrullinated peptide antibody (anti-CCP), if RA is suspected. The specificity of anti-CCP underlies the rationale for checking RF and anti-CCP concurrently. We aim to understand the current practices of Polyarthritis work up in primary care physicians. (PCPs)
Methods: A cross-sectional survey was created via Redcap and administered to PCPs – Staff and Resident, across the Cleveland Clinic Enterprise in November 2019. It enquired about physician demographics, practice characteristics, knowledge and physician-reported ordering practices related to patients presenting with polyarthritis. We reviewed data from our electronic medical record (Epic) through the use of slicer-dicer, in order to identify patients with ICD-10 codes for Polyarthritis seen in the primary care setting between 9-2018 and 9-2019 and associated orders placed by providers. Statistical analysis was completed using descriptive statistics and Fisher’s exact test of independence to find relationships between.
Results: The survey was sent to 325 physicians with a 28% response rate; the demographics of the 92 survey respondents are described in Table 1. Slicer-dicer data from EPIC showed RF was ordered 30% more than anti-CCP. Self-reported survey reveals similar discordance with 32% of respondents reported they would order both an RF and anti-CCP, and 33% would order only an RF. Both staff and residents report being unfamiliar with the guideline-based workup of polyarthritis (Table 2). Most respondents reported ordering an ESR and CRP (83% and 79%, respectively), with 64% of respondents selected RF and 39% selected anti-CCP in the initial work-up of polyarthritis (Table 3). There was a statistically significant association between physician-reported evidence-based ordering of both an RF and anti-CCP with respondents being staff physicians (P ≤ 0.001) and self-reported knowledge of guidelines (P ≤ 0.001).
Conclusion: Physician-reported and observational EMR data suggest that the workup of polyarthritis in the primary care setting, as it relates to the ordering of RF and anti-CCP antibodies, is frequently incongruent with ACR recommendations. Guideline-discordant ordering practices are more common with residents and in those who report lacking knowledge of the guidelines. This suggests that physician experience and knowledge are the most likely underlying drivers of guideline-based workups of polyarthritis in the primary care clinic. We plan to address this issue by building an order set into our EMR that will provide decision support to promote workups of polyarthritis congruent with the ACR recommendations, thereby improving knowledge and practice.
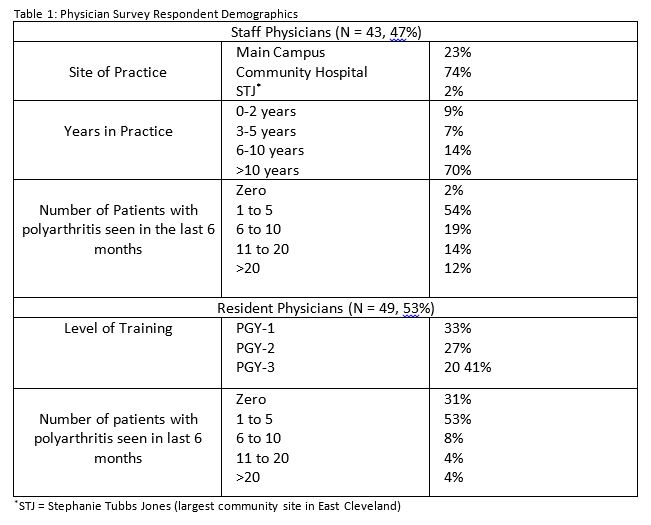 Table 1 : Physician Survey Respondent Demographics . @STJ = Stephanie Tubbs Jones
Table 1 : Physician Survey Respondent Demographics . @STJ = Stephanie Tubbs Jones
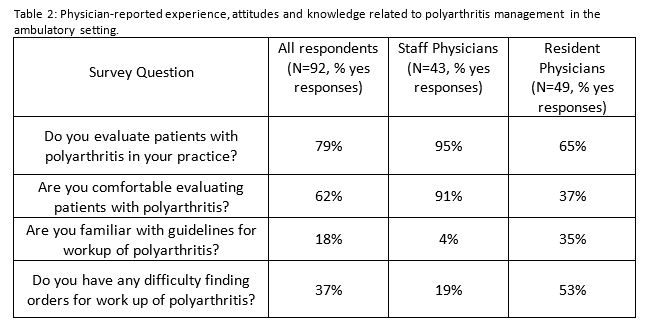 Table 2: Physician-reported experience, attitudes and knowledge related to polyarthritis management in the ambulatory setting.
Table 2: Physician-reported experience, attitudes and knowledge related to polyarthritis management in the ambulatory setting.
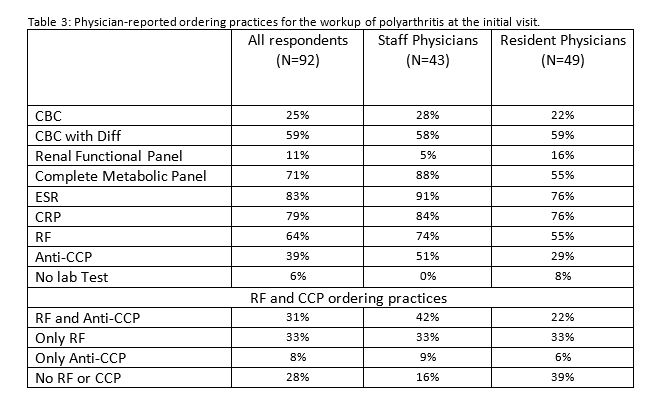 Table 3: Physician-reported ordering practices for the workup of polyarthritis at the initial visit.
Table 3: Physician-reported ordering practices for the workup of polyarthritis at the initial visit.
To cite this abstract in AMA style:
Desai R, Calabrese C, Patel N, Donato J. Polyarthritis Workup in Primary Care Setting : How Are We Doing? [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/polyarthritis-workup-in-primary-care-setting-how-are-we-doing/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/polyarthritis-workup-in-primary-care-setting-how-are-we-doing/