Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Pleuroparenchymal Fibroelastosis (PPFE) is a rare idiopathic interstitial pneumonia characterized by fibrosis of the visceral pleura and subpleural parenchyma, predominantly affecting the upper lobes. PPFE can be seen in the context of including infections, post-transplant, and sometimes, or association with connective tissue diseases (CTDs). When in seen with CTDs, PPFE has been reported commonly in patients with systemic sclerosis, followed by rheumatoid arthritis, and to a lesser extent, Sjogren syndrome, inflammatory myopathies, and ANCA-associated vasculitis. This study aims to present a retrospective analysis of patients presenting with PPFE associated with CTD-associated interstitial lung disease (CTD-ILD), with comparisons among CTDs.
Methods: We performed a retrospective study focused on patients diagnosed with PPFE and CTD-ILD seen at Mayo Clinic from January 1, 2000, to November 30, 2023. We performed a search in our electronic data extraction tool with the following terms: “pleuroparenchymal fibroelastosis” and “systemic sclerosis”, “SLE”, “mixed connective tissue disease” “dermatomyositis/polymyositis”, “Sjogren syndrome”, “rheumatoid arthritis”, “antiphospholipid syndrome”, “vasculitis”, and “ankylosing spondylitis”. The diagnosis of PPFE was confirmed as reported by radiologists based on characteristic findings on computed tomography (CT). The CTD diagnosis was based on documentation by a rheumatologist. We performed descriptive statistics to describe the characteristics and findings of our cohort. Differences by group were tested using Kruskal-Wallis and Fisher’s exact tests.
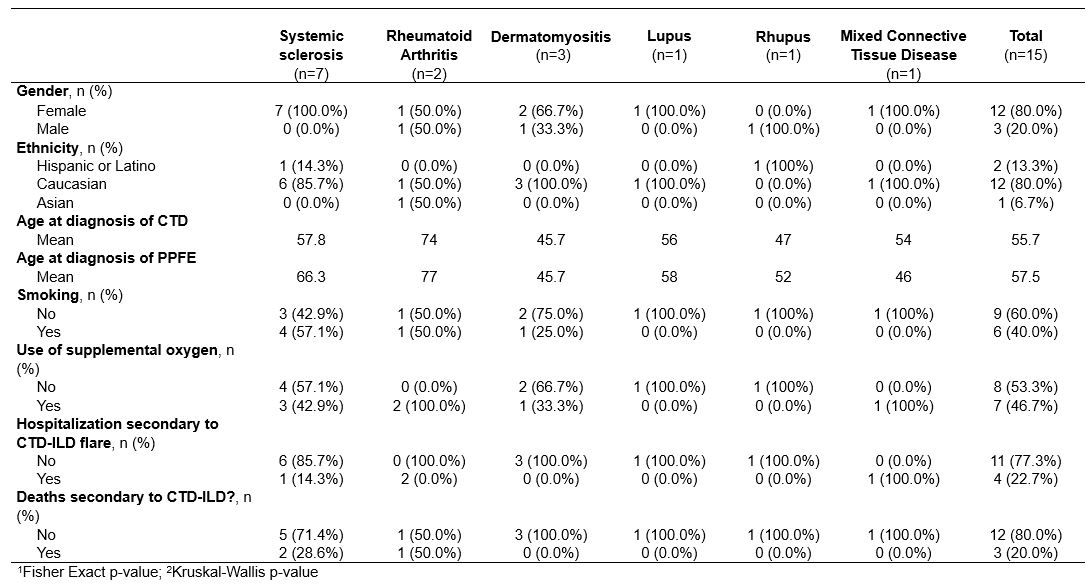
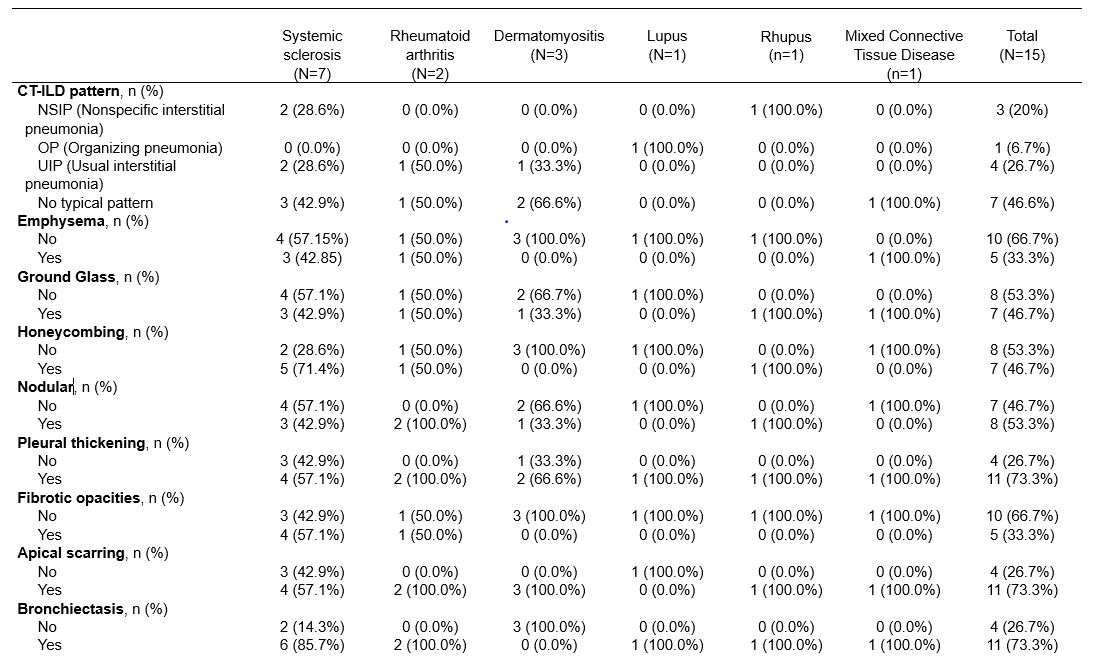
Results: A total of 110 patients were reviewed based on the search criteria, and 15 patients met the criteria for PPFE and CTD-associated ILD. Among these patients (Table 1), 7 had systemic sclerosis, 3 had dermatomyositis, 2 had rheumatoid arthritis, 1 had systemic lupus erythematosus (SLE), 1 with rhupus and 1 mixed connective tissue disease. The association was predominantly seen in female, with only 3 out of 15 patients being male across all groups. The median age of diagnosis of the CTD was 55.7 years, and 57.5 years old at the diagnosis of PPFE. Smoking history was noted in all four groups, accounting for 40.0% of the total 15 patients. Oxygen requirements were present in 46.7% of patients overall Radiological findings on CT scans are included in Table 2. Hospitalizations due to ILD flares were reported in 4 out of 15 patients. Mortality occurred in 3 out of 15 patients, with 2 deaths among those with systemic sclerosis and 1 among those with rheumatoid arthritis.
Conclusion: In our cohort of CTD patients with PPFE the majority had systemic sclerosis, consistent with previous reports in the literature. Notably, we identified a novel occurrence of PPFE in systemic lupus erythematosus (SLE) and mixed connective tissue disease, which warrants further investigation due to its previously unreported nature. Further exploration of PPFE characteristics in other groups such as idiopathic pulmonary fibrosis (IPF) could help us differentiate the phenotype and outcomes between the two groups (PPFE in IPF versus PPFE in CTD-ILD).
To cite this abstract in AMA style:
Diaz Menindez M, Diaz Arumir Vergara A, Shing V, mead harvey c, Zamora Martinez A, Nagaraja V. Pleuroparenchymal Fibroelastosis Associated with Connective Tissue Diseases (PPFE-CTD) [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/pleuroparenchymal-fibroelastosis-associated-with-connective-tissue-diseases-ppfe-ctd/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/pleuroparenchymal-fibroelastosis-associated-with-connective-tissue-diseases-ppfe-ctd/