Session Information
Date: Tuesday, November 9, 2021
Title: Abstracts: Epidemiology & Public Health II: Inflammatory Arthritis (1923–1926)
Session Type: Abstract Session
Session Time: 3:45PM-4:00PM
Background/Purpose: Rheumatoid arthritis (RA) leads to substantial healthcare utilization and premature mortality. Prior work has demonstrated that the overlapping presence of comorbid chronic conditions, termed multimorbidity, is a primary driver of these long-term outcomes. However, optimal methods to assess multimorbidity in RA in the clinical setting are not established. For example, traditional comorbidity indices (e.g. Charlson Comorbidity Index, Rheumatic Disease Comorbidity Index [RDCI]) have little clinical utility. Therefore, we aimed to derive informative multimorbidity clusters that could be readily applied in the day-to-day care of patients with RA.
Methods: We constructed RA cohorts within a large commercial insurance database (MarketScan) and the Veterans Health Administration (VA) between 2006 and 2015 using validated administrative algorithms for RA. Pre-selected chronic conditions (n=42) were identified using diagnosis codes from outpatient and inpatient encounters. We performed k-means clustering of factor analysis scores (reflecting morbidity patterns) that were generated from the aforementioned chronic conditions independently in both datasets. Associations of unique cluster assignment with healthcare utilization (number of inpatient, emergency room [ER], and outpatient encounters) over up to 5 years was evaluated separately in both datasets using generalized estimating equations models adjusting for age and sex. In the VA, we also used multivariable Cox regression models to compare survival between clusters adjusting for age, sex, race, smoking status, and calendar year.
Results: From the multimorbidity patterns, we identified 4 distinct patient clusters in MarketScan (n=113,425) and 3 clusters in the VA (n=32,640) based on cubic clustering criterion (Figure 1). Based on the frequency of chronic conditions present, we identified “low”, “moderate”, and “severe” multimorbidity clusters. Patients in the “moderate/severe” multimorbidity clusters were older, more frequently male, and had higher RDCI and Charlson scores (Table 1). A cluster characterized by mental health and chronic pain diseases was also identified in both datasets. Referent to the “low” multimorbidity cluster, patients in the other clusters had significantly higher rates of inpatient, ER, and outpatient encounters (Table 2). In VA survival analyses, 9,415 deaths occurred over 228,534 patient-years of follow-up. Crude mortality rates were higher in both multimorbid clusters, but after multivariable adjustment, only the mental health and chronic pain cluster was significantly associated with higher mortality (HR 1.11 [95% CI 1.04, 1.18]).
Conclusion: Machine-learning approaches identified meaningful multimorbidity clusters among RA patients in two independent real-world datasets. Our approach highlights mental health and chronic pain multimorbidity, a pattern not accounted for in some widely used comorbidity indices, as a key determinant of long-term outcomes in RA. By retaining the ability to predict health outcomes with the simplicity of a cluster group assignment, this approach represents a crucial step forward in assessing multimorbidity at the point of care in clinical settings.
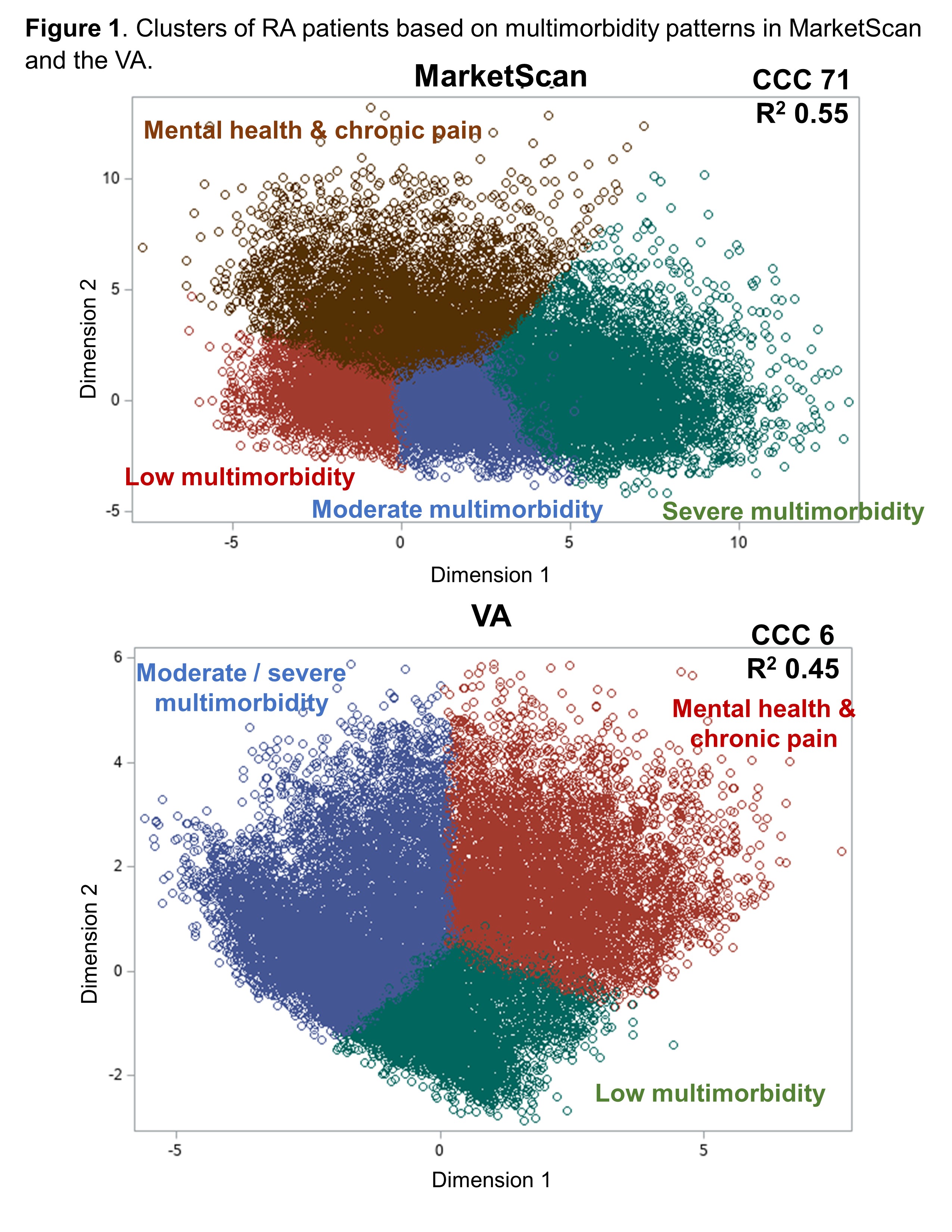 Figure 1. Clusters of RA patients based on multimorbidity patterns in MarketScan and the VA. Clustering of RA patients in both datasets performed using k-means clustering of factor analysis scores derived from the presence of 42 chronic conditions. Abbreviations: CCC, cubic clustering criterion
Figure 1. Clusters of RA patients based on multimorbidity patterns in MarketScan and the VA. Clustering of RA patients in both datasets performed using k-means clustering of factor analysis scores derived from the presence of 42 chronic conditions. Abbreviations: CCC, cubic clustering criterion
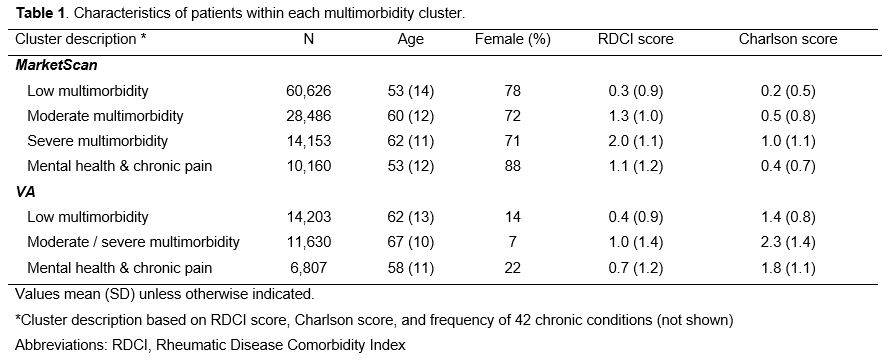 Table 1. Characteristics of patients within each multimorbidity cluster
Table 1. Characteristics of patients within each multimorbidity cluster
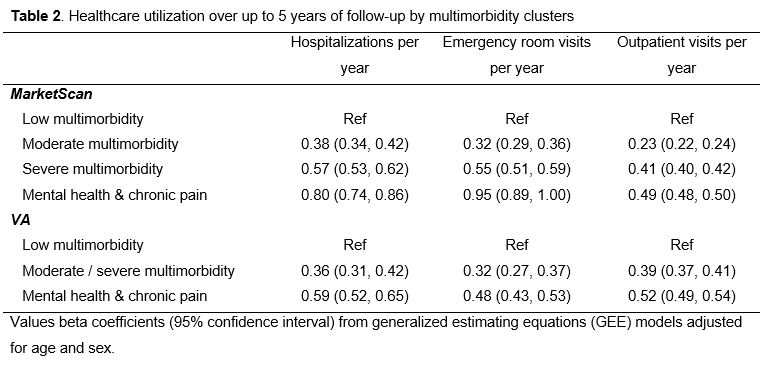 Table 2. Healthcare utilization over up to 5 years of follow-up by multimorbidity clusters
Table 2. Healthcare utilization over up to 5 years of follow-up by multimorbidity clusters
To cite this abstract in AMA style:
England B, Yang Y, Roul P, Haas C, Sayles H, Yu F, Sauer B, Baker J, Michaud K, Curtis J, Mikuls T. Patient Clustering Based on Multimorbidity Patterns Predicts Healthcare Utilization and Mortality in Rheumatoid Arthritis Within Independent Real-World Datasets [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/patient-clustering-based-on-multimorbidity-patterns-predicts-healthcare-utilization-and-mortality-in-rheumatoid-arthritis-within-independent-real-world-datasets/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/patient-clustering-based-on-multimorbidity-patterns-predicts-healthcare-utilization-and-mortality-in-rheumatoid-arthritis-within-independent-real-world-datasets/