Session Information
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Pain in myositis is poorly studied and multifactorial relating to muscle weakness, arthritis, myofasciitis, fibromyalgia or other co-morbidities. We sought to prospectively evaluate patient-reported pain, cross-sectionally and longitudinally in association with the collection of myositis core set measures of disease activity, patient reported and functional measures.
Methods: In a prospective, longitudinal observational study, we enrolled 50 myositis patients [dermatomyositis (DM), polymyositis (PM), necrotizing myositis (NM), and anti-synthetase syndrome (AS)] from February 2016 to April 2018. Patients with fibromyalgia and severe arthritis (except from myositis) were excluded. All subjects had a baseline and 6-month visit, where all myositis core set measures (CSM) [muscle enzymes, manual muscle testing (MMT-9), patient and physician (MD) global disease activity, extra-muscular disease activity and HAQ-DI], functional measures [Timed up and go (TUS), Sit to Stand (STS), 6 Minute Walk Distance (6-MWD)] and patient-reported outcomes [PROMIS-physical function (PF) and SF-36] were evaluated. Further, a standard 10 cm visual analogue scale(VAS) for pain and fatigue were recorded at both visits. A score between 0-3 was considered mild, >3-7 moderate, and >7-10 as severe pain. The phenotypic and disease activity measures of the cohort were correlated with pain (Spearman) at baseline visit. Longitudinal changes in pain at 6 months were correlated with the CSM and the functional and patient-reported outcomes. The change in pain was also evaluated if it improves with the published 2016 ACR/EULAR myositis response criteria graded as no, minimal, moderate or major improvement and the MD and patient global assessment of change. Strength of correlation was defined as weak (0.1-0.29), moderate (0.3-0.49) or strong (≥0.5).
Results: Twenty-four patients had DM, 9 NM, 6 PM and 11 AS with a mean age, 51.6 (±14.9) with 60% (n=30) females. The mean (SD) of pain was 2.7 (2.6), with 55.1% having mild pain, 40.8 % moderate pain and 4.08% severe pain at baseline. There was no significant difference in pain by disease subsets (DM vs. non-DM), autoantibody status, age at diagnosis or enrollment, or BMI. Pain was associated with having muscle weakness (MMT), disease duration and showed trends for association with active disease (as per MD) and female gender. At baseline, pain showed a strong correlation with fatigue, patient-reported disease activity, HAQ-DI, PROMIS PF, SF36 and aldolase and a moderate correlation with muscle weakness (MMT), MD global disease activity and 6MWD. Longitudinal analyses suggested that changes in pain showed a moderate to strong correlation with MD global disease activity, patient-reported disease activity, fatigue, SF36 and functional measures (TUG and STS). Pain improved significantly in patients with a moderate to major improvement, and similar non-significant trends were seen for the physician and patient reported change.
Conclusion: Pain in myositis is typically of mild to moderate severity and is moderately associated with the CSM and improves over time particularly in subjects demonstrating a moderate to major clinical response in published outcome metrics.
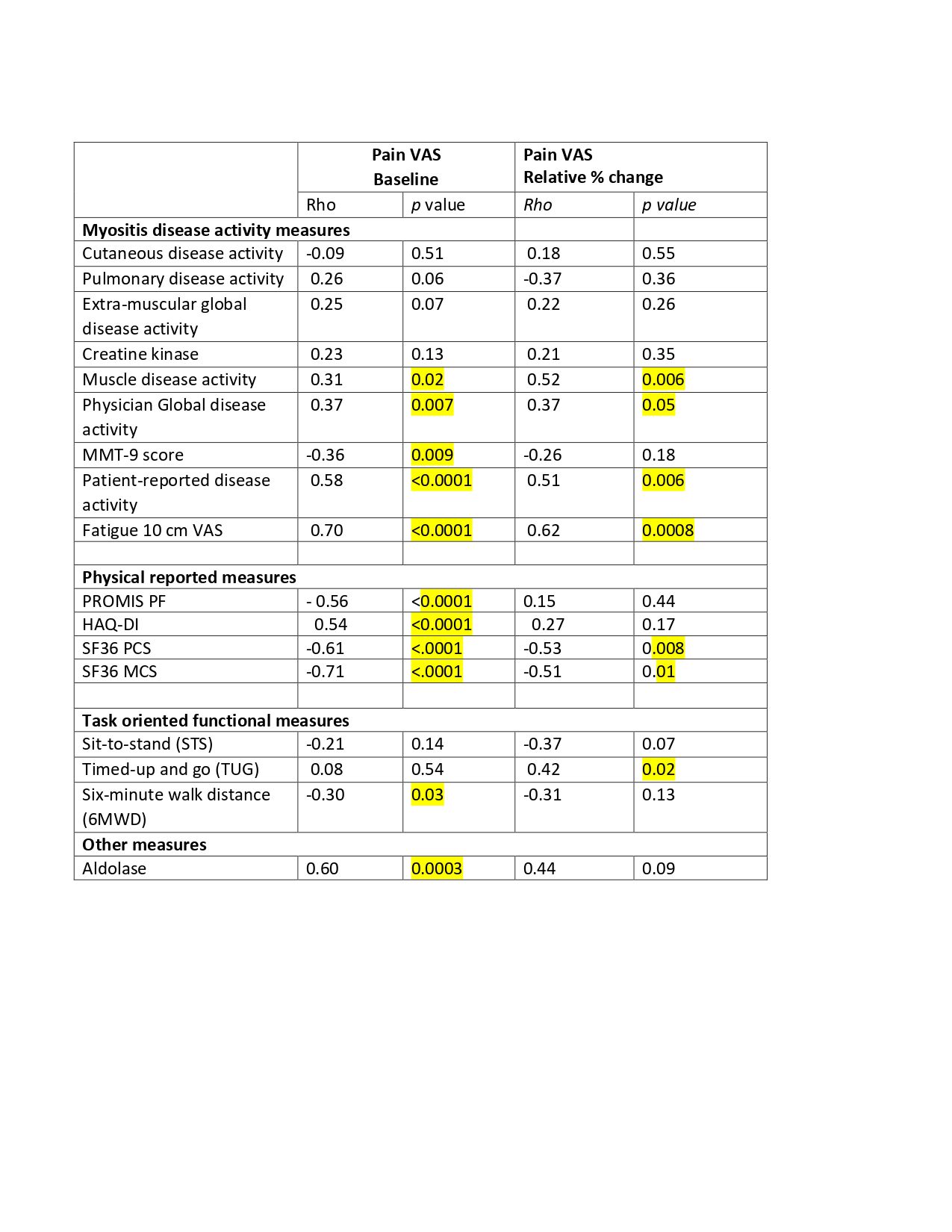 Table 1: Correlation of pain by VAS with myositis disease activity, functional and patient-reported outcomes at baseline and longitudinal change at 6 months.
Table 1: Correlation of pain by VAS with myositis disease activity, functional and patient-reported outcomes at baseline and longitudinal change at 6 months.
 Figure 1: Relative percent change in VAS pain scores related to the ACR-EULAR myositis response criteria.
Figure 1: Relative percent change in VAS pain scores related to the ACR-EULAR myositis response criteria.
To cite this abstract in AMA style:
Chandrasekhara Pillai A, Oddis C, Moghadam-Kia S, Ascherman D, Neiman N, Koontz D, Dianxu R, Aggarwal R. Pain in Myositis Is Associated with the Disease Activity [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/pain-in-myositis-is-associated-with-the-disease-activity/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/pain-in-myositis-is-associated-with-the-disease-activity/