Session Information
Date: Tuesday, November 12, 2019
Title: Miscellanous Rheumatic & Inflammatory Disease Poster III: Autoimmune Conditions and Therapies
Session Type: Poster Session (Tuesday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Pachymeningitis is a rare complication of rheumatic disease. Patients present with hearing loss or other neurologic complications. Diagnosis is made by thickening of dura or leptomeninges on MRI-imaging or histopathologically with biopsy of the dura. The prevalence pachymeningitis in rheumatic disease is unknown, and there is no standard of care.
Methods: We retrospectively identified nine patients diagnosed with pachymeningitis based on clinical symptoms, MRI findings, and in three cases, dural biopsy. We assessed the rheumatologic diagnoses, presenting symptoms, treatment modalities, and outcomes.
Results: There were two males and seven females, with a mean age of 63 for males and 60 for females. Five patients had rheumatoid arthritis, two had sarcoidosis, one had undifferentiated connective tissue disease and Sjogren’s syndrome, and one had blastomycosis who developed rheumatoid arthritis one year later. The presenting symptoms were hearing loss (three), unilateral weakness (two), unilateral numbness (two), seizure (two). Additional symptoms included headache, confusion, memory loss, tinnitus, scleritis, optic neuritis, unilateral hemineglect, foot flaccidity, and gait disturbance. Diagnosis was confirmed in three patients with dural biopsy. MRI images were obtained on all patients. Six patients were treated solely with prednisone or pulse-dose methylprednisolone. Two patients were treated with anti-TNF agents and one patient with rituximab. Pre- and post-treatment MRI demonstrated resolution of leptomeningeal abnormality in two patients. Six out of nine patients reported resolution of symptoms with treatment. Three had persistent deficits, including hearing loss, visual impairment, and slight residual hemiplegia.
Conclusion: Rheumatoid arthritis was the most common rheumatological diagnosis, and hearing loss was the most common presenting symptom. Most patients had resolution of symptoms with prednisone, pulse methylprednisolone, anti-TNF agents, or rituximab. We hope this case series will assist clinicians with the diagnosis and management of pachymeningitis.
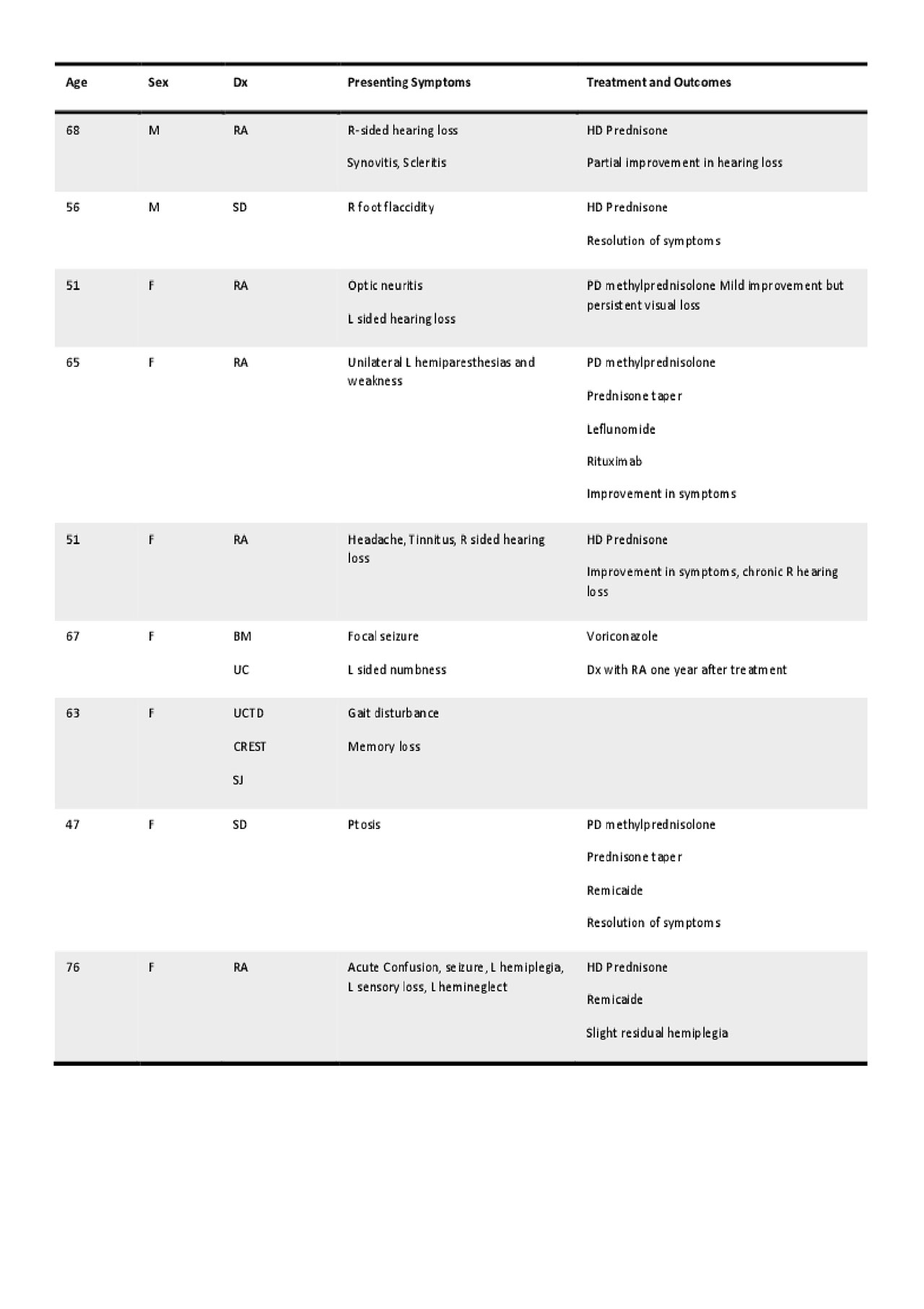
Table 1

Figure 1
To cite this abstract in AMA style:
Kneeland R, Berry J, Brandwein S, Starosta M. Pachymeningitis in Rheumatic Disease [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/pachymeningitis-in-rheumatic-disease/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/pachymeningitis-in-rheumatic-disease/