Session Information
Date: Monday, November 13, 2023
Title: (1442–1487) SLE – Diagnosis, Manifestations, & Outcomes Poster II
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Up to 50% of patients suffering from systemic lupus erythematosus (SLE) develop lupus nephritis (LN) within the first 10 years of diagnosis and 5 to 20% of them progress to end-stage kidney disease (ESKD) (1,2). Several poor prognostic factors have been identified, such as the presence of tubulointerstitial and/or vascular lesions, a high chronicity index (3), African American descent (4), hypertension (5), absence of renal remission (3),(5) and renal flare(s) (6). Obesity, per se, is a risk factor for chronic kidney disease (CKD).Thus, obesity-related glomerulopathy in patients with a body mass index (BMI) ≥30kg/m2(7)progresses to CKD in up to 50% of the cases (8). In addition, obesity is a risk factor for progression of primary glomerular diseases, such as IgA nephropathy (IgAN) (9). Whether obesity contributes to CKD risk in LN has never been investigated, to the best of our knowledge. We took advantage of the Louvain LN Inception cohort to test this hypothesis.
Methods: We retrospectively studied 132 patients with biopsy-proven class III, IV or V incident LN followed for a median period of 140 months (min. 25). Remission was defined as a urine protein to creatinine (uP:C) ratio < 0.5 g/g and a serum creatinine value < 120% of baseline. Renal relapse was defined as the reappearance of a uP:C >1 g/g, leading to a repeat kidney biopsy and treatment change. Poor long-term renal outcome was defined as the presence of CKD. Unpaired t-tests, Wilcoxon’s signed rank tests, chi-square tests, Fisher’s exact tests, log-rank test and Cox regression were used as appropriate.
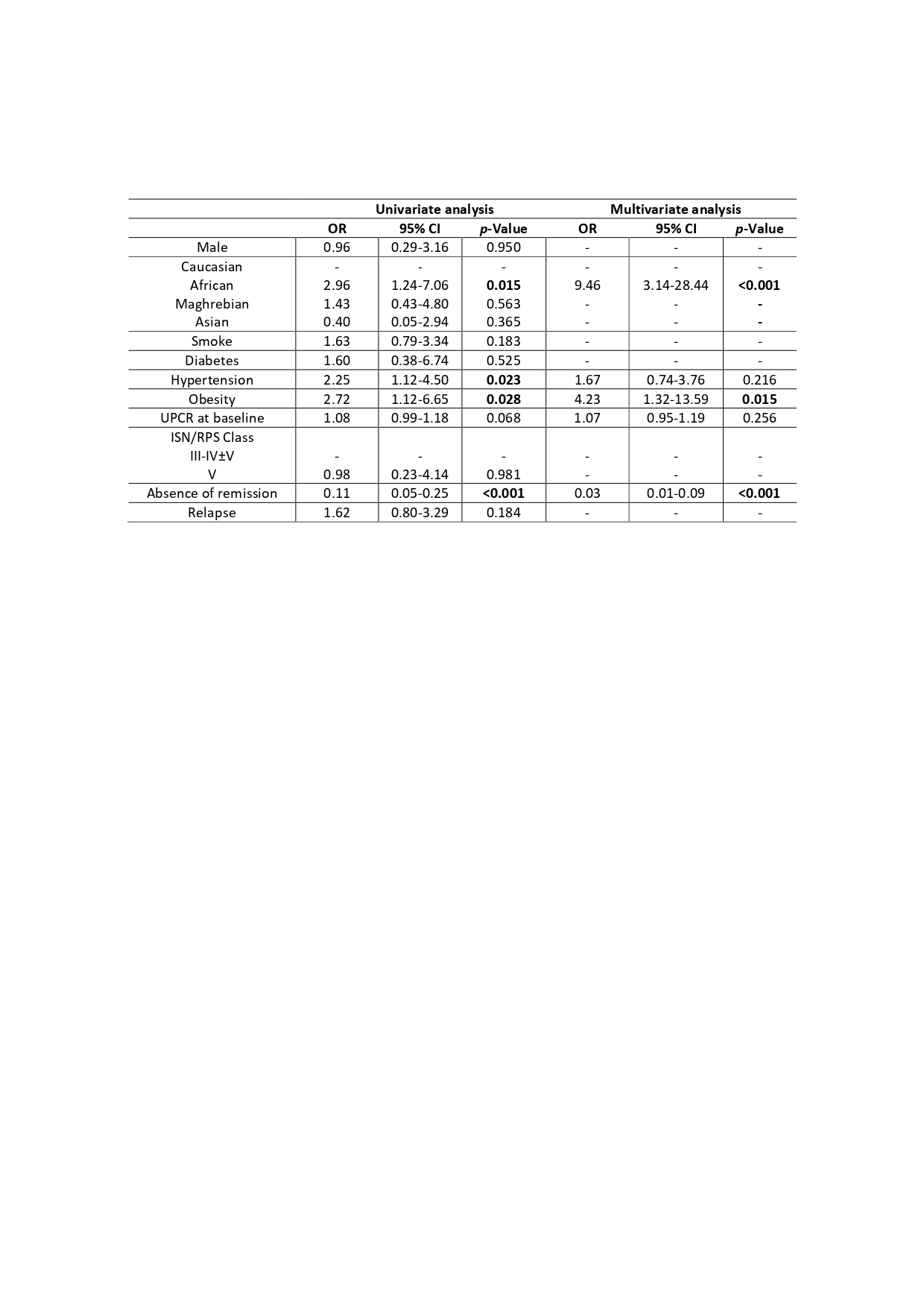
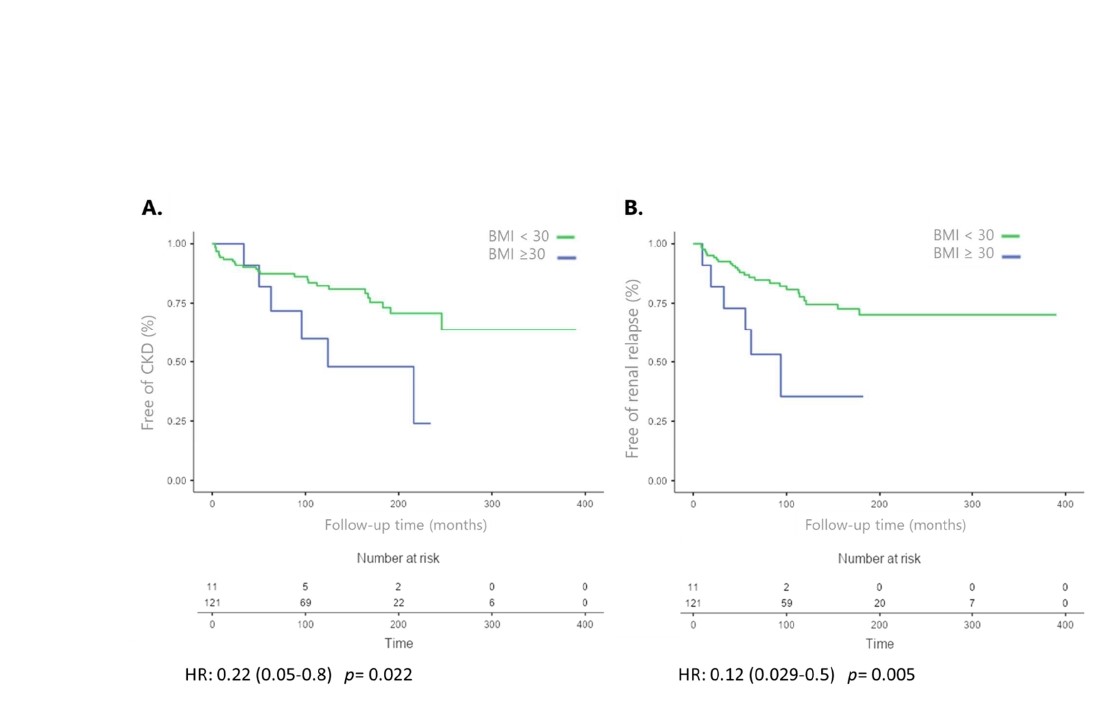
Results: The majority of patients were women (89%) and Caucasian (70.5%). Thirty-two patients (24%) developed CKD. Their baseline characteristics did not differ from those without CKD. Nine patients (6.8%) developed ESKD. Eleven patients (8.3%) suffered from obesity, defined by a body mass index (BMI) ≥30kg/m2. Of note, “dry” weight was considered for patients presenting with oedema related to nephrotic syndrome. None of the obese patients was pregnant at disease onset. Renal remission was achieved in 90% of the cases, but 54% relapsed. Only one obese patient died from lupus-related macrophage activation syndrome. Obesity significantly increased long-term CKD risk [OR= 4.23 (IC95% 1.32-13.59), p = 0.015]. As shown in Table 1, obesity was an independent risk factor of CKD, as were African descent and absence of remission. Time-to-CKD and time-to-renal relapse were shorter in obese patients compared to non-obese patients (Fig 1). By Cox regression, factors independently associated with CKD were African descent, hypertension, absence of remission and obesity, as shown in Table 1.
Conclusion: A BMI ≥30 kg/m2 is an independent poor prognostic factor for CKD in LN and is associated with shorter time to renal relapse. More attention should therefore be paid to weight control in LN patients.
To cite this abstract in AMA style:
Cuervo Gutiérrez F, Enfrein A, Houssiau F, Tamirou F. Obesity Is an Independent Poor Prognostic Factor in Lupus Nephritis [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/obesity-is-an-independent-poor-prognostic-factor-in-lupus-nephritis/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/obesity-is-an-independent-poor-prognostic-factor-in-lupus-nephritis/