Session Information
Date: Sunday, November 13, 2022
Title: Systemic Sclerosis and Related Disorders – Clinical Poster II
Session Type: Poster Session C
Session Time: 1:00PM-3:00PM
Background/Purpose: Fibroproliferative vasculopathy in systemic sclerosis (SSc) is caused by neointima proliferation is a key pathologic feature of SSc which results in arterial vessel narrowing (e.g., through adventitial fibrosis) and contributes to microvascular injury and damage. The aim of our study was to determine the value of non-contrast MRI-based DAVIX in predicting digital ulcers (DUs) and worsening of patient reported outcomes (PROs)/clinical manifestations in SSc.
Methods: 91 consecutive patients with Raynaud’s phenomenon were enrolled in this study.
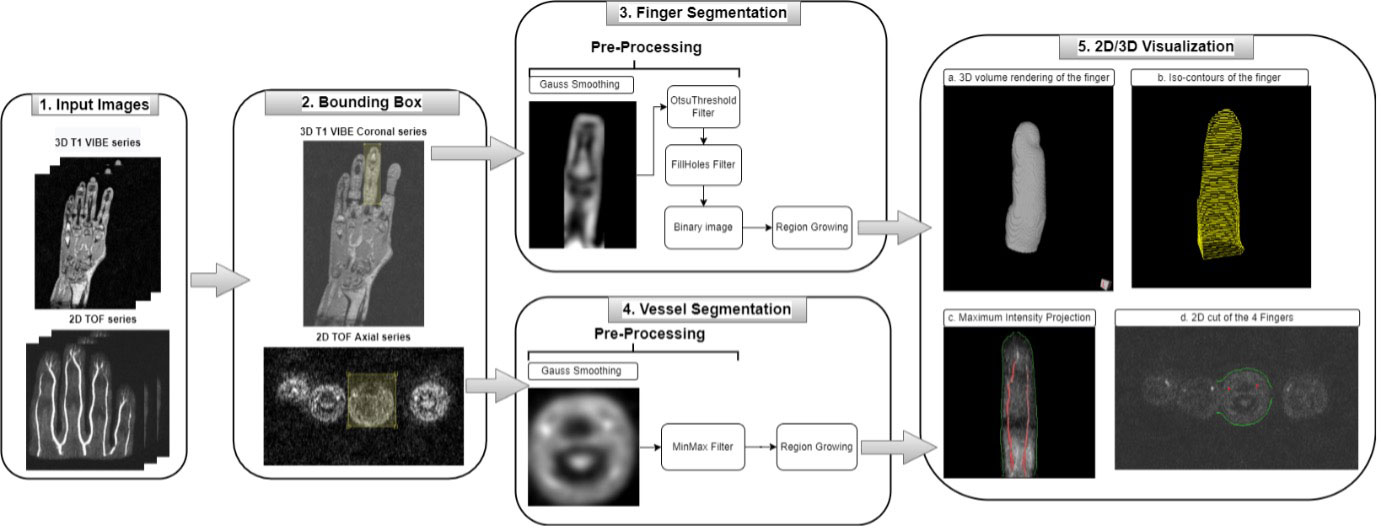
At baseline, patients underwent an MRI scan of their dominant hand. We utilised a time-of-flight MR angiography (TOF) sequence which allows the visualization of vessels by the enhancement of flowing blood and the suppression of surrounding stationary tissue in a definite volume (Figure 1). Briefly, our method uses a region growing algorithm to semi-automatically detect the arteries and the finger anatomy (Figure 1). DAVIX of the dominant hand was calculated as %mean of the 4 fingers.
Data collected included (but was not limited to): pulmonary function tests, nailfold capillaroscopy, modified Rodnan Skin Score (mRSS), history/presence of DU, and sHAQ-DI.
The distribution of data was analysed with D’Agostino-Pearson normality test. Medians were compared by Mann-Whitney-Wilcoxon test, correlation with clinical manifestations was performed using Spearman’s or Pearson test, as appropriate using Prism 7, GraphPad Software. Correlation between DAVIX and capillaroscopy was scored as a semi quantitative integer scale ranging from 0 to 4 (normal, non-specific, early, active, late).
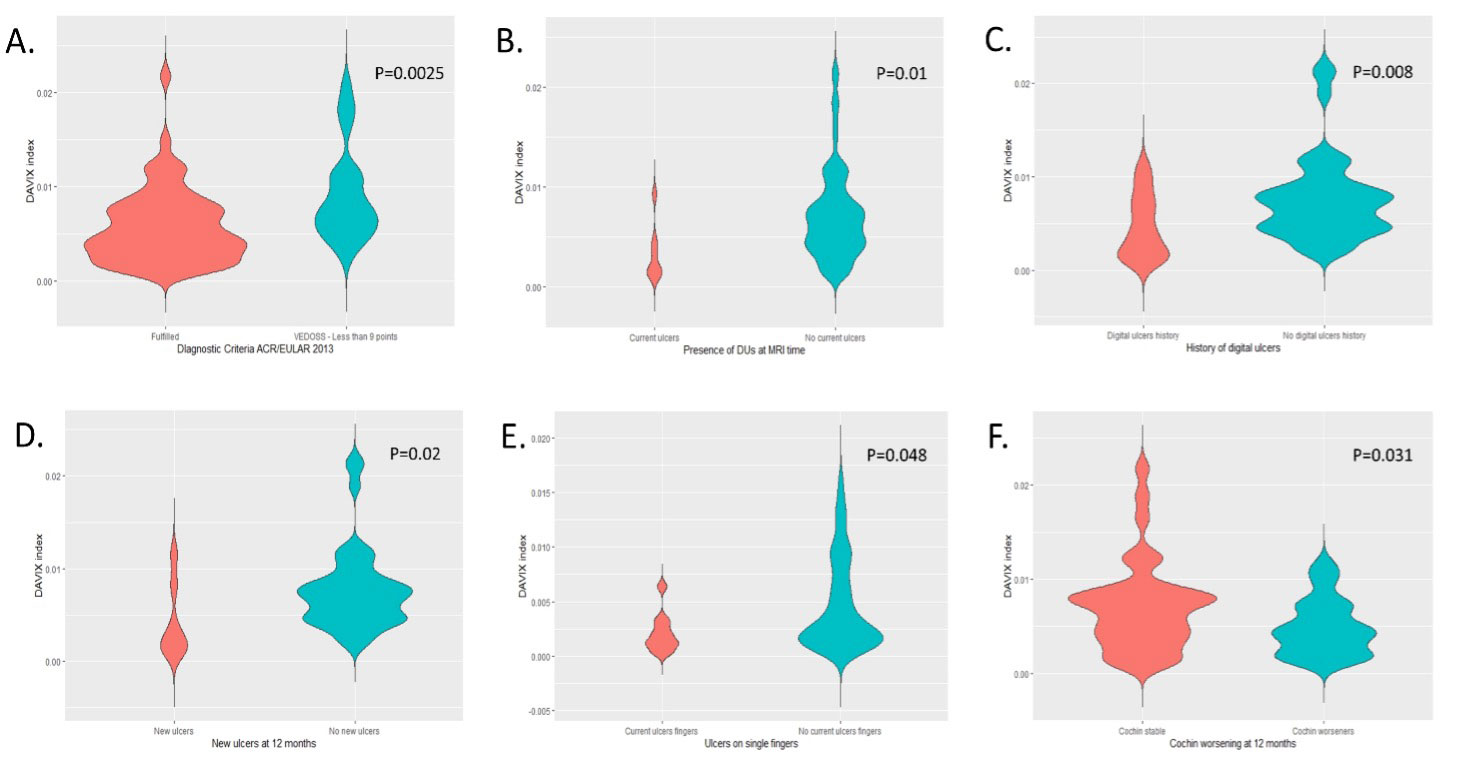
Results: The majority (86%) were females, 62 fulfilled 2013 SSc classification criteria with 5.9 (7) years median (IQR) disease duration. Twenty-nine were patients with VEDOSS (mRSS Score < 9). Complete historical and prospective (12-month) follow-up data were available for 85 patients. Patients fulfilling SSc criteria had a lower median (IQR) DAVIX compared to those with VEDOSS [0.46% (0.48) vs 0.75% (0.54), P=0.0025] (Figure 2).
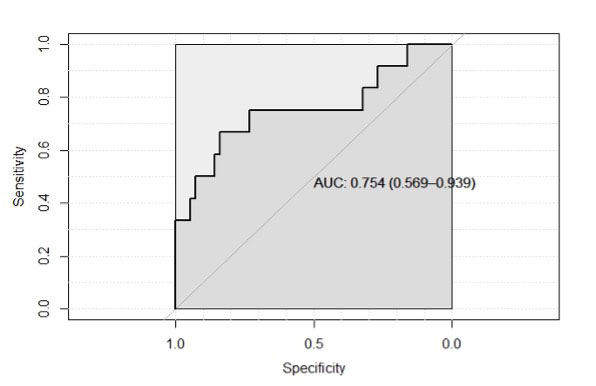
DAVIX was significantly lower in patients with DUs at baseline (P=0.01) and in those with DU history (P=0.008) (Figure 2). Further, in the group with no previous/current DU, DAVIX of patients who developed new DUs during follow-up was 0.23% vs. 0.66% (P=0.02) (Figure 2). ROC curve analysis (Figure 3) indicated that a DAVIX threshold < 0.36% conferred a 4 times higher risk of new DUs.
DAVIX correlated with disease duration (r=-0.415, P< 0.0001), baseline mRSS (r=-0.278, P=0.028), DLCO% (r=0.368, P=0.004), FVC/DLCO (r=-0.337, P=0.009), and capillaroscopy pattern (r=-0.447, P< 0.001). Additionally, DAVIX correlated with worsening HAQ-DI (r=-0.308, P=0.024), Raynaud (r=-0.270, P=0.048) and DU VAS (r=-0.291, P=0.044).
Conclusion: DAVIX is a promising surrogate outcome measure of vascular disease in SSc. The predicative value of DAVIX to predict worsening of PROs and future DUs may be useful for patient enrichment/stratification in clinical trials and offer insights into vascular disease activity in SSc disease progression.
To cite this abstract in AMA style:
Hughes M, Di Donato S, Gjeloshi K, Abignano G, Danzo F, Lettieri G G, De Lorenzis E, Bertham D, O’Connor P, Kubassova O, Del Galdo F. MRI Digital Artery Volume Index (DAVIX) Predicts Future Digital Ulcers and Disease Progression in Systemic Sclerosis [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/mri-digital-artery-volume-index-davix-predicts-future-digital-ulcers-and-disease-progression-in-systemic-sclerosis/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/mri-digital-artery-volume-index-davix-predicts-future-digital-ulcers-and-disease-progression-in-systemic-sclerosis/