Session Information
Date: Tuesday, November 14, 2023
Title: (1913–1944) Miscellaneous Rheumatic & Inflammatory Diseases Poster III
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Anti-synthetase syndrome (ASS) is a chronic autoimmune inflammatory condition, characterized by myositis, interstitial lung disease (ILD), arthritis, Raynaud’s phenomenon and mechanic’s hands. This systematic review (SR) aims to summarise the manifestations, management and outcomes of ILD associated with ASS (ASS-ILD).
Methods: The protocol was registered on Prospero (CRD42023416414). Articles discussing management and outcomes of ASS-ILD, published 1946 until April 2023, were included. Medline, Embase and Cochrane Databases were searched. Case reports, case series of < 10, reviews and conference abstracts were excluded. Articles meeting inclusion criteria were examined by two authors. Data on demographics, treatment, antibody serology, physiological and radiological findings at baseline and one-year were extracted.
Results: Initially, 451 articles were retrieved with 10 included (9 cohort, 1 case series; Figure 1). Risk of bias assessment established studies were of variable quality (Table 1). A total of 514 patients were included, 67.8% female, mean age 52.4 (SD 4.6) years at ILD induction therapy. Cohorts were from: Europe (n=5); North America (n=3); China (n=2). Patients had the following myositis-associated autoantibodies: Jo-1 (48%); PL7 (15.1%); PL12 (29.2%), EJ (15.9%); OJ (3.3%). In addition, 143 patients had anti-Ro52 positivity. Baseline high-resolution computed tomography (where available) showed: non-specific interstitial pneumonia (NSIP) (n=220; 42.8%); organising pneumonia (OP) (n=142; 27.6%); NSIP/OP overlap (n=51; 9.9%); nonspecific interstitial pneumonia (n=34; 6.6%). Of these, NSIP subtype was reported in 12 patients (6 fibrotic, 6 cellular). Pulmonary hypertension was discussed in 2 cohorts, with 6 patients having a confirmed diagnosis. Patients received the following drugs for induction (with glucocorticoids [GC]): cyclophosphamide (CYC) (n=136; 26.5%); rituximab (RTX) (n=88; 17.1%); calcineurin inhibitors (n=84; 16.3%); other disease-modifying anti-rheumatic drugs (n=183; 35.6%); intravenous immunoglobulin (IVIG; n=17; 3.3%); GC only (n=20; 3.9%). Overall median forced vital capacity (FVC) pre-treatment was 52.7% and 68.5% at one year. Overall median diffusion capacity of lungs for carbon monoxide (DLCO) pre-treatment was 44.5% and 49.1% at one year. Due to heterogeneity of methodology and cohorts, direct comparison was not possible for most drugs. Patients treated with RTX had an overall median 12.2% improvement in FVC and 2.9% increase in DLCO at one year. Patients treated with CYC had a 17% and 6.3% increase in FVC and DLCO respectively after one year. In patients receiving IVIG, 7/17 had >10% increase in FVC at one year. 5.4% (n=28) were reported to have died post-treatment due to: infection (n=8) including Pneumocystis [n=2, both post-rituximab]; malignancy (n=3); multiorgan failure (n=2). 15 patients had no reported cause of death.
Conclusion: This is the first SR summarising the management and outcomes of ASS-ILD. No significant difference was found between the effectiveness of treatments with regards to physiological respiratory function. More robust trials are required to reduce the morbidity and mortality resulting from ASS-ILD.
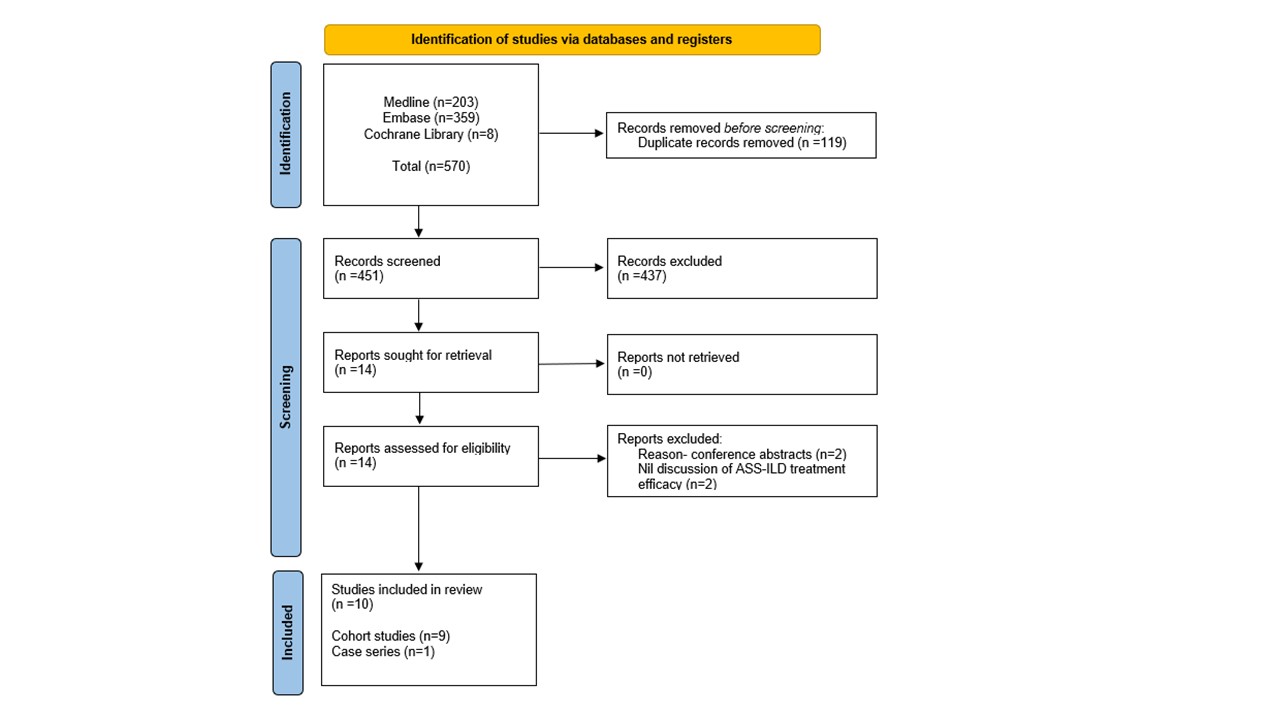
Flow diagram of stages of systematic literature review.
Cochrane Library encompasses library of: systematic reviews; systematic review protocols; controlled clinical trials. ASS-ILD: interstitial lung disease associated with anti-synthetase syndrome.
To cite this abstract in AMA style:
Kouranloo K, Dey M, Yioe V, Spencer L, Cotton C. Manifestations, Management and Outcomes of Interstitial Lung Disease Associated with Anti-synthetase Syndrome: A Systematic Literature Review [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/manifestations-management-and-outcomes-of-interstitial-lung-disease-associated-with-anti-synthetase-syndrome-a-systematic-literature-review/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/manifestations-management-and-outcomes-of-interstitial-lung-disease-associated-with-anti-synthetase-syndrome-a-systematic-literature-review/