Session Information
Session Type: Poster Session A
Session Time: 1:00PM-3:00PM
Background/Purpose: Paraoxonase 1 (PON1) is a high-density lipoprotein (HDL)- associated enzyme with antioxidative properties, which is low in activity in patients with idiopathic inflammatory myopathies (IIM) compared to controls (S. Bae et al. 2021 PMID 34698804). Low PON1 activity exposes subjects to higher oxidative stress which has been shown to activate carcinogenic pathways (J.N. Molony et al. 2018, PMID 28587975). The current work evaluates PON1 activity in IIM patients with and without cancer.
Methods: PON1 activity was assessed in baseline visit specimens of patients who entered a longitudinal single center IIM cohort. PON1 enzyme activity was assessed by paraoxonase, arylesterase and lactonase assays (C. Charles et al. 2020 PMID 33033318) and was compared between patients with and without cancer. Diagnosis of cancer excluded non-melanoma skin cancers. Multivariate logistic regression models examined the association between PON1 activity and cancer diagnosis.
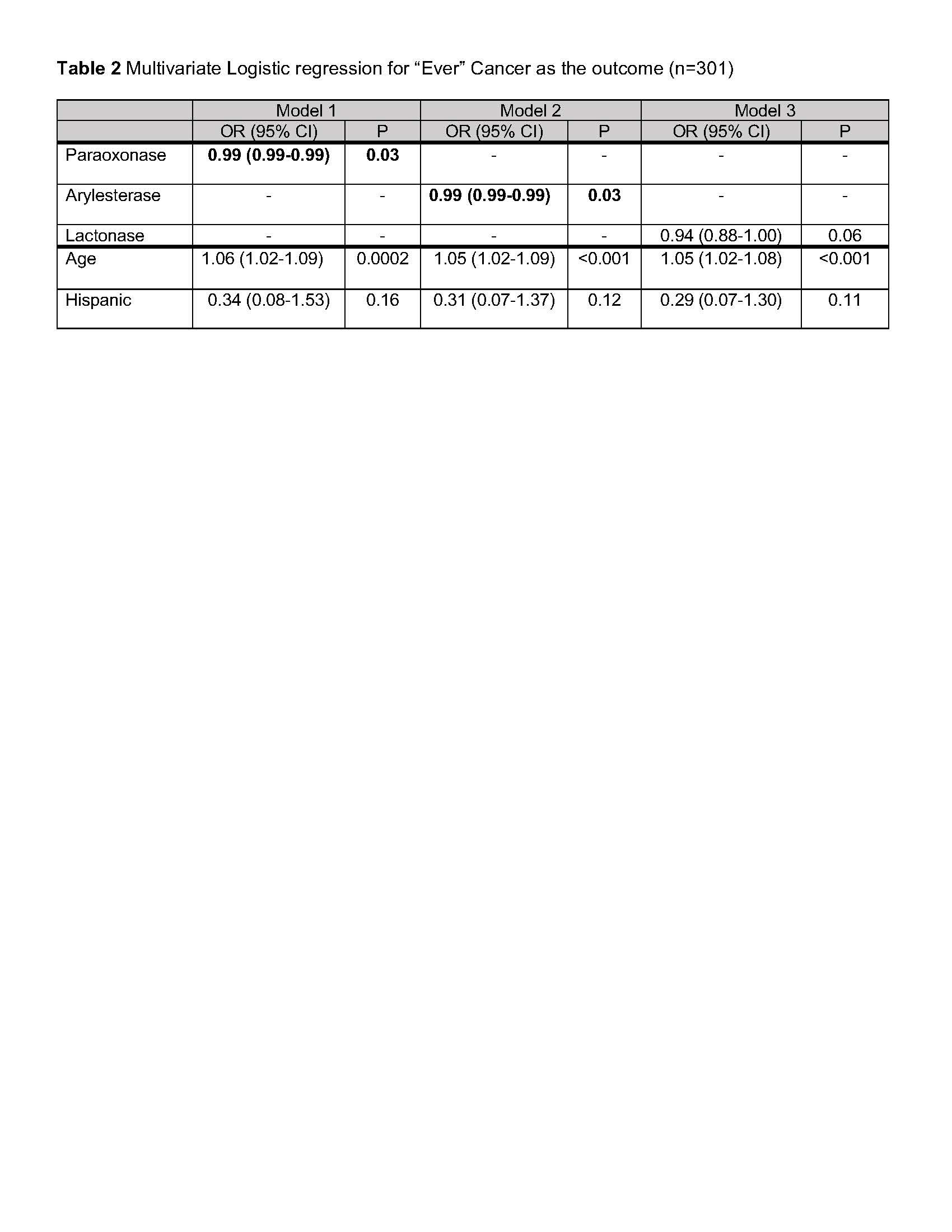
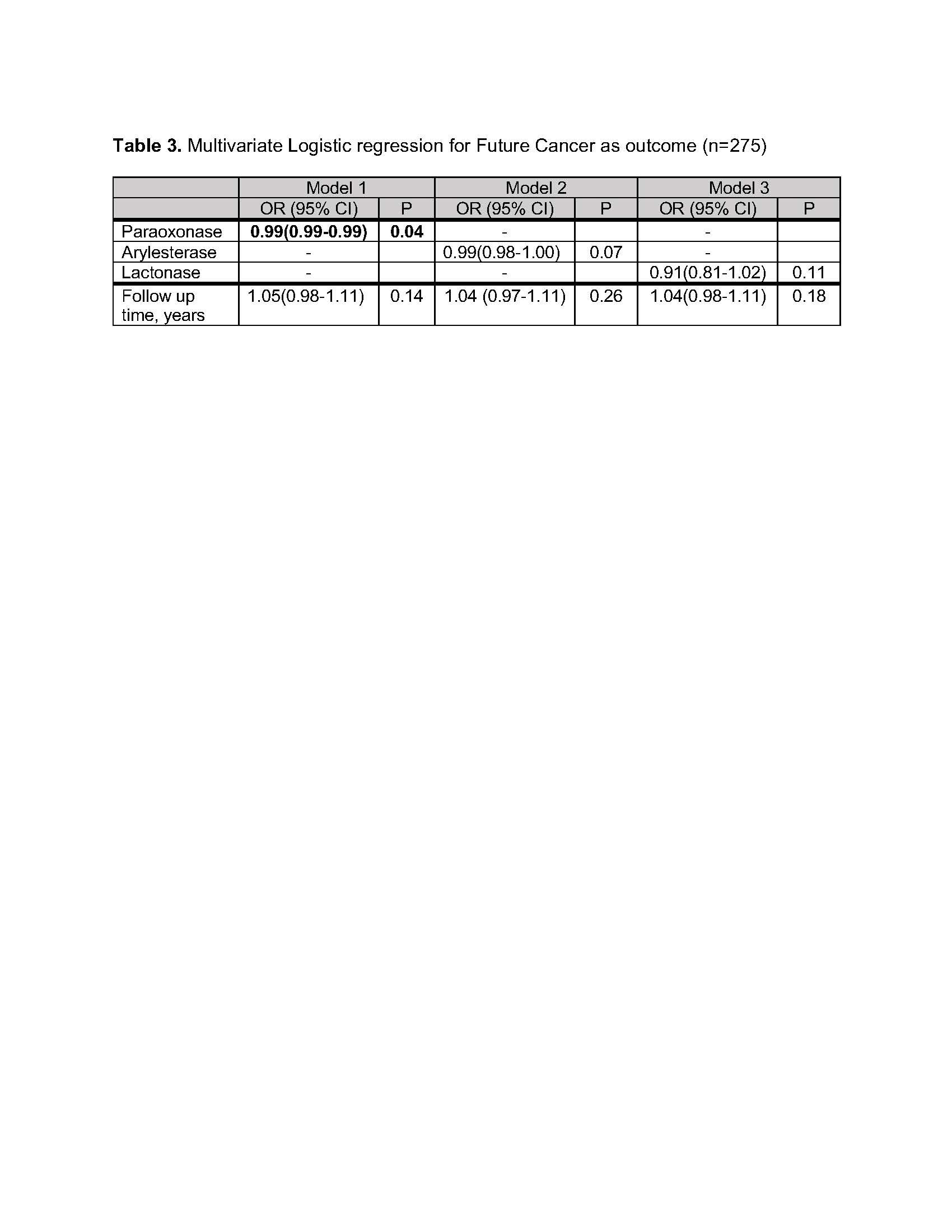
Results: 36 out of 301 IIM patients (12%) had an “ever” diagnosis of cancer including 16 patients with cancer prior to IIM diagnosis, 10 patients with cancer after IIM diagnosis and prior to cohort entry, and 10 patients with cancer after IIM diagnosis and after cohort entry. The most common cancer types were breast 12(33%) and prostate (22%). In analysis of the entire cohort, patients with “ever” cancer were older and less likely to be Hispanic compared to patients without cancer. Other clinical characteristics including IIM type, myositis autoantibodies, and physician global disease activity scores were similar between the groups (Table 1). PON1 enzyme activity was significantly lower in patients with “ever” cancer compared to patients without cancer by all 3 assays. This association remained statistically significant in multivariate logistic regression controlling for significant variables in bivariate analyses for both paraoxonase and arylesterase activities (Table 2). In analysis of the 10 patients who developed cancer after cohort entry (Table 1), baseline PON1 activity by the paraoxonase assay also predicted cancer development after model adjustment for follow up time; similar trends were noted for arylesterase and lactonase models (Table 3). Patients with active cancer at the time of blood draw (n=8) had the lowest PON1 activities compared to those with either treated or future cancers (n=28) and those without cancer (arylesterase activity: active cancer,134[28] U/ml; treated or future cancer, 175 [62] U/ml; no cancer 207[83] U/ml, mean [SD] for all, p< 0.05 for both compared to no cancer group, paraoxonase and lactonase show similar trends).
Conclusion: PON1 enzyme activity is suppressed in IIM patients with a diagnosis of “ever” cancer, and also associates with future cancer diagnosis in a single center cohort. Future multicenter studies are needed to elucidate the role of PON1 in cancer development in IIM and to further evaluate it as a potential risk biomarker.
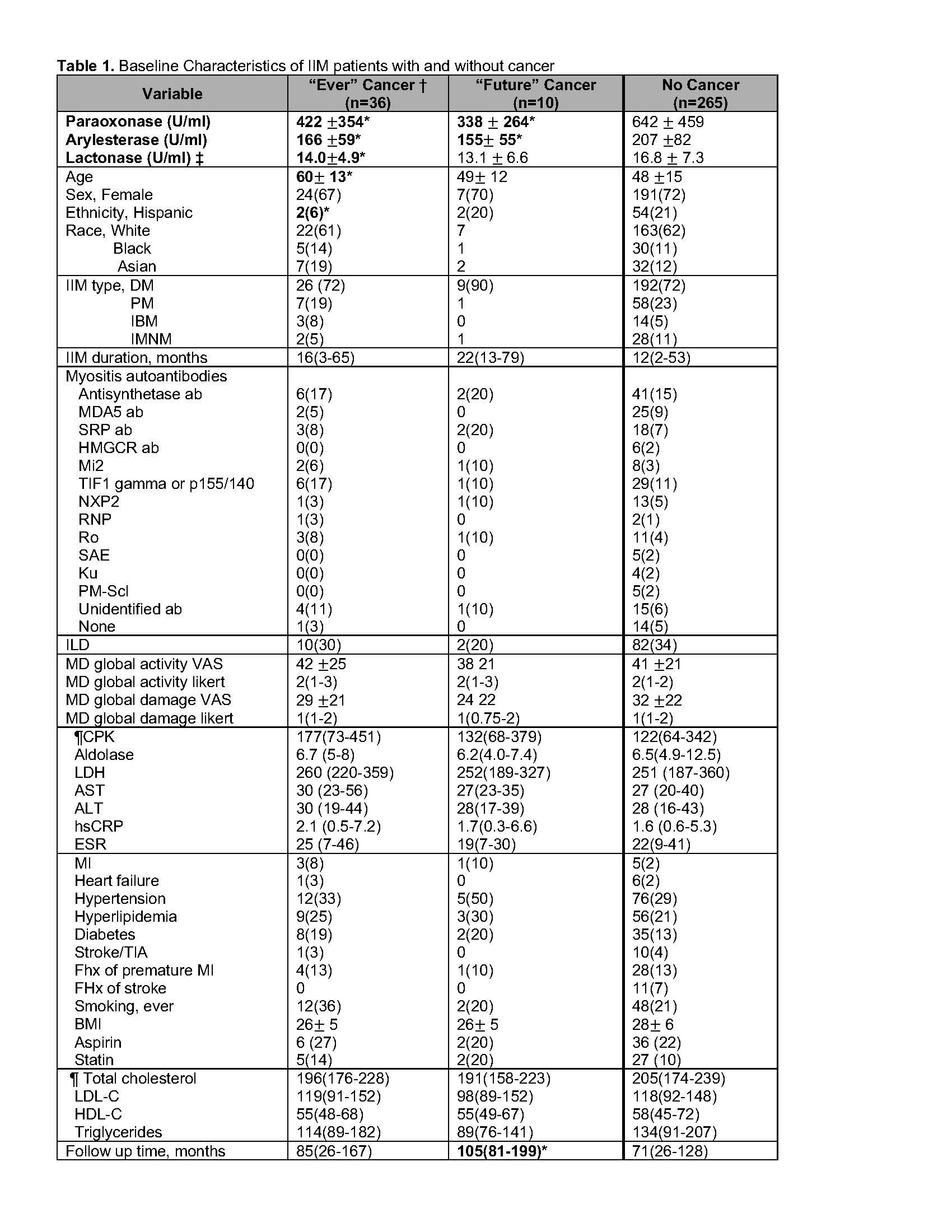
*p<0.05 compared to No Cancer group
†Ever Cancer did not include patients with pre-cancerous lesion, benign tumors, non-melanomatous skin cancer
‡ Lactonase missing in 9 patients
¶ Labs missing in 31 patients, lipid panel missing in 36 patients
To cite this abstract in AMA style:
Bae S, Shahbazian A, Wang J, Charles-Schoeman C. Low Paraoxonase-1 Enzyme Activity in Patients with Idiopathic Inflammatory Myopathies Associates with Cancer Diagnosis [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/low-paraoxonase-1-enzyme-activity-in-patients-with-idiopathic-inflammatory-myopathies-associates-with-cancer-diagnosis/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/low-paraoxonase-1-enzyme-activity-in-patients-with-idiopathic-inflammatory-myopathies-associates-with-cancer-diagnosis/