Session Information
Session Type: Poster Session D
Session Time: 9:00AM-11:00AM
Background/Purpose: High body mass index (BMI, kg/m2) is a modifiable risk factor that has been associated with the development and progression of osteoarthritis (OA) and knee pain. While total knee arthroplasty (TKA) is the gold standard for the treatment of end stage OA, morbidly obese patients (BMI≥40kg/m2) are often required to lose weight prior to TKA due to increased surgical risk and a higher rate of complications. While conservative weight-loss often fails to help these patients, bariatric surgery can be an alternative option. Here we present interim data from the trial entitled “Surgical Weight-loss to Improve Functional Status Trajectories following arthroplasty for painful knee osteoarthritis”. This current multi-center, prospective study compares pain and functional outcomes in patients receiving bariatric surgery prior to TKA versus obese patients who go straight to TKA.
Methods: Patients with BMI ≥40 kg/m2 and painful knee osteoarthritis who met the indications for TKA were recruited at four hospital centers. Patients with a BMI >35 kg/m2 were also recruited if they had a qualifying comorbid condition including obstructive sleep apnea, diabetes, hypertension or hyperlipidemia. Patients were assigned to either the bariatric (BAR) or TKA arm based on surgical choice (goal n=150 for each arm), with all bariatric patients having anatomy-altering sleeve gastrectomy or gastric bypass. At baseline and several time points after surgery (Figure 1), we documented height, weight, the Knee injury and Osteoarthritis Outcome Score (KOOS), visual analog pain (VAS) scales, and the Western Ontario and McMaster Universities Arthritis Index (WOMAC), and had patients perform functional assessments (Timed-Up and Go, 30-second Chair Stand and 40-meter fast paced walk test). We targeted minimum detectable change (MDC) in outcomes for the VAS for knee pain (33% reduction), Timed Up and Go (decrease by 2 seconds), 30-second Chair Stand (increase by 2 reps), 40-meter fast paced walk (increase by 0.16 m/s), WOMAC score (16% reduction), and the KOOS pain score (10-point improvement). Using a logistic regression to adjust for age and baseline BMI, we compared the percentage of patients in the two arms who achieved an MDC for the various outcomes.
Results: To date, 25 BAR and 28 TKA patients have completed their follow-up visits through at least 6 months. Although there was a similar sex distribution, the bariatric group was younger (52 vs 60 years old, p=0.0023) with a higher baseline BMI (47.0 vs 41.6 p=0.0006). Most bariatric patients achieved comparable improvement to the TKA cohort with regards to the benchmarks of the 30-second Chair Stand (TKA 54% vs BAR 33%, p=0.156), KOOS pain score (TKA 91% vs BAR 67%, p=0.130), the Visual Analog Pain Scale (TKA 50% vs BAR 39%, p=0.466), Timed Up and Go test (TKA 43% vs BAR 22%, p=0.141) and the 40-meter fast paced walk (TKA 61% vs BAR 35%, p=0.073). The TKA cohort had a greater percent with a MDC for the WOMAC (TKA 88% vs BAR 54%, p=0.030).
Conclusion: In morbidly obese patients who are eligible for TKA, bariatric surgery may result in modest improvements in knee outcomes and may eventually delay the need for a TKA.
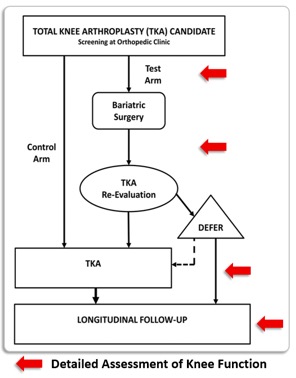 Figure 1. Study flowchart
Figure 1. Study flowchart
To cite this abstract in AMA style:
Samuels J, Zak S, Schwarzkopf R, Ren-Fielding C, Parikh M, McLawhorn A, Browne J, Hallowell P, Irving B, Wood C, Still C, Benotti P. Knee OA Outcomes in Patients with Severe Obesity Following Bariatric Surgery or Total Knee Arthroplasty [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/knee-oa-outcomes-in-patients-with-severe-obesity-following-bariatric-surgery-or-total-knee-arthroplasty/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/knee-oa-outcomes-in-patients-with-severe-obesity-following-bariatric-surgery-or-total-knee-arthroplasty/