Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Semi-quantitative scoring systems have long been used for radiographic findings in osteoarthritis (OA), but limited work has utilized ultrasound (US). The aim of this study was to utilize a rigorous approach based on factor analysis and nonparametric item response theory (IRT) to determine whether a single US summary score is appropriate for knee OA assessment.
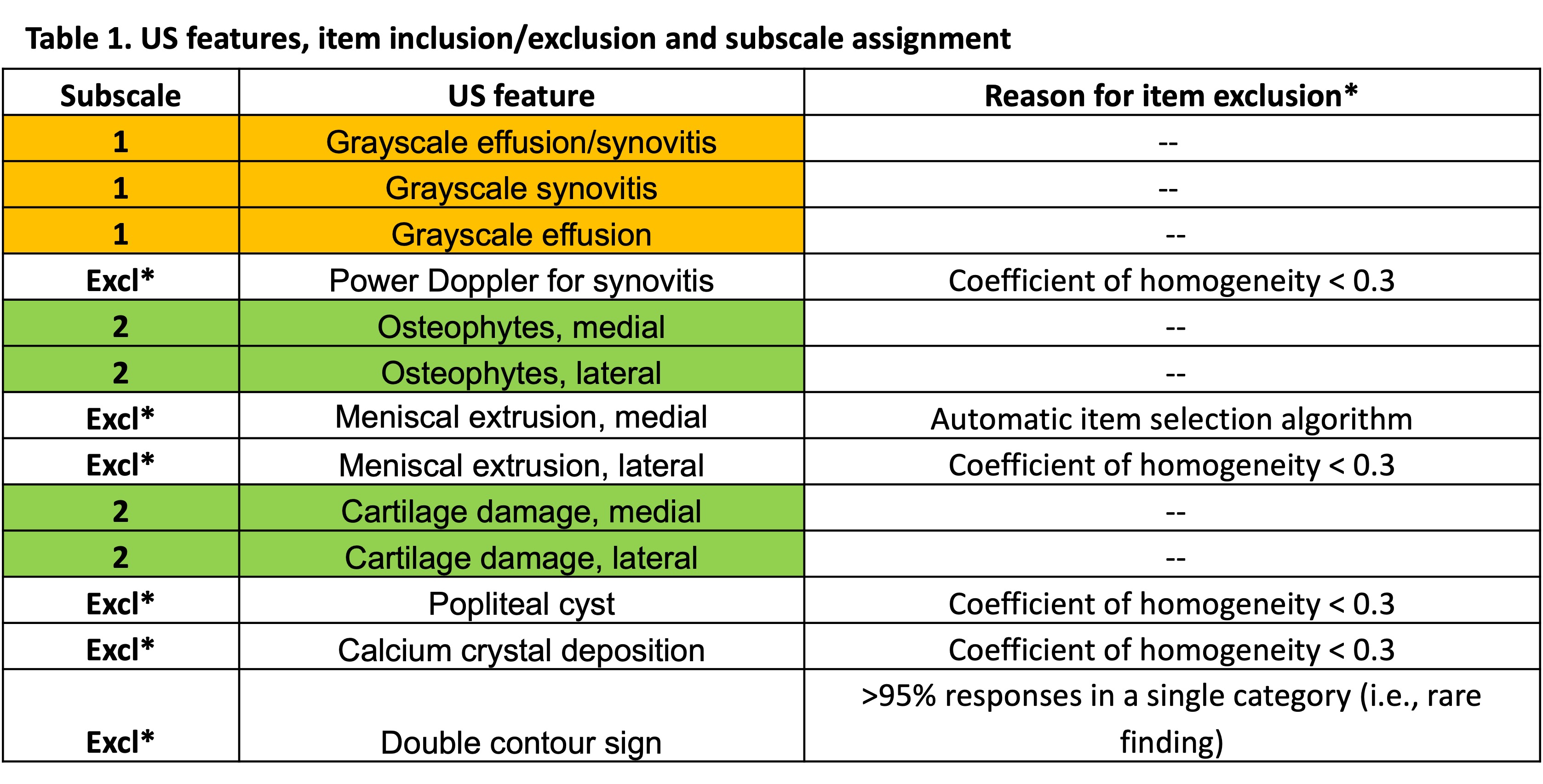
Methods: Data were from Johnston County Health Study (JoCoHS) participants who underwent standardized radiography and ultrasonography of bilateral knees (PMID39989271). Symptomatic knee OA (sxKOA) was defined as a Kellgren-Lawrence grade of 2 or more in a knee with self-reported symptoms. A series of iterative procedures, i.e., Principal Components Analysis (PCA), Parallel Analysis (PA), Item Cluster Analysis (ICA), Very Simple Structure analysis (VSS), Confirmatory Factor Analysis (CFA), Mokken Scaling Analysis (MSA), and Classical Test Theory, were used to derive final items and subscales from US features (Table 1). In CFA, we considered the comparative fit index (CFI), the Tucker–Lewis index (TLI), and the root mean square error of approximation (RMSEA). MSA examines coefficients of homogeneity for items (Hi) and scale (H) and explores possible dimensionality solutions. Monotonicity, scalability, and invariant ordering of any determined subscales were also assessed.
Results: Complete data for 13 US features were available for 824 of 902 JoCoHS participants (91%); 33% were male, 39% had sxKOA, mean age 55 ± 10 years and mean BMI 33 ± 8 kg/m2. After exclusions based on test diagnostics and outliers, 791 participants and 12 items (all but double contour) remained for analyses. Items with the lowest Hi were removed one by one, and the analyses were repeated until Hi and H were above 0.3. H was 0.356 when all 5 problematic items were excluded (7 items remained, Table 1). The PA, ICA, and VSS analysis on 8 and 7 items suggested 2 factors, but were inconsistent regarding the inclusion of medial meniscal extrusion. As the PCA loadings for this item were low, and its inclusion reduced reliability, we determined that the optimal number of items was 7, and the number of subscales was two (Table 1). The 2-factor CFAs of the 7-item model produced CFI and TLI = 0.99; RMSEA = 1.16. The coefficients of homogeneity were 0.747 for Subscale 1 (3 items) and 0.452 for Subscale 2 (4 items).Since only Subscale 2 met all criteria, a composite score was derived for the second subscale only, demonstrating a linear relationship with KL grade for both females and males (Figure 1).
Conclusion: A robust composite score could be applied in clinical and research settings where only US is available or is preferred. The 4 US features in Subscale 2 form a moderate to strong Mokken scale, enabling persons to be ordered using a summary score. Future work will investigate Subscale 1 and the reason for MSA assumptions violation given that the three grayscale US features form a strong Mokken scale (H >=0.5). These results demonstrate that US summary score development and validation can benefit from both CFA and nonparametric IRT. Parametric IRT will be used to diagnose fit further and for scoring algorithm development.
.jpg)
To cite this abstract in AMA style:
Arbeeva L, Alvarez C, Samuels J, Lin J, Kohler M, Bakewell C, Schwartz T, Nelson A. Item Response Theory to Develop an Ultrasound Composite Score for Knee Osteoarthritis Assessment [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/item-response-theory-to-develop-an-ultrasound-composite-score-for-knee-osteoarthritis-assessment/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/item-response-theory-to-develop-an-ultrasound-composite-score-for-knee-osteoarthritis-assessment/