Session Information
Date: Monday, October 27, 2025
Title: (1191–1220) Muscle Biology, Myositis & Myopathies – Basic & Clinical Science Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Systemic autoimmune rheumatic diseases (SARDs) are a major cause of interstitial lung disease (ILD), with high prevalence in inflammatory idiopathic myopathy (IIM), systemic sclerosis (SSc), and rheumatoid arthritis (RA). In clinical practice, ILD assessment relies primarily on high-resolution CT (HRCT), as surgical lung biopsy is infrequently performed in SARDs-ILD. This study aims to evaluate the correlation between radiologic patterns at diagnosis and histopathologic findings in explanted lung tissue from SARDs-ILD patients undergoing lung transplantation.
Methods: Patients with ILD secondary to IIM, SSc, or RA who underwent lung transplantation between January 1, 2014 and April 30, 2024 at Vancouver General Hospital and between January 1, 2012 and December 31, 2024 at the Centre hospitalier de l’Université de Montréal were included. Agreement between HRCT and histologic diagnoses was assessed using kappa (κ) statistics with predefined coefficient weights: complete agreement (same diagnoses, κ=1), partial agreement (overlapping terms, for example, NSIP vs. NSIP/UIP κ=0.5), or no agreement (different terms, κ=0). The HRCT-histopathology relationship was visualized using an Alluvial chart (Flourish, UK).
Results: The study included 70 patients (18 IIM, 24 SSc, and 28 RA) (Table 1). RA patients were older at transplant, more likely to have a smoking history, and less likely to be female compared to IIM and SSc. IIM patients were more likely to require emergency lung transplant. At initial presentation, nonspecific interstitial lung disease (NSIP) was the predominant HRCT pattern in IIM (55.6%) and SSc (75%) patients, while usual interstitial lung disease (UIP) was most common in RA (57.1%) (Table 2). On explant pathology, NSIP remained the primary tissue diagnosis in SSc (62.5%), followed by mixed NSIP/UIP (20.8%) and UIP (12.5%). In RA, UIP was the most frequent histopathologic pattern (50%), followed by mixed NSIP/UIP (25%) and NSIP (17.9%) (Table 2). Cohen’s κ analysis with custom coefficient weight demonstrated moderate agreement between HRCT and histology for SSc (κ = 0.42, p=0.02) and RA (κ = 0.46, p=0.002). In contrast, IIM showed insignificant correlation (κ = 0.14, p=0.4), with explant pathology distributed across all six diagnostic patterns. Notably, 50% of IIM patients undergoing transplant had anti-MDA5 dermatomyositis with rapidly progressive ILD clinically, and either diffuse alveolar damage (DAD) or unclassifiable end stage fibrosis on explant.
Conclusion: This study demonstrates moderate radiologic-histologic correlation in SSc- and RA-associated ILD. However, IIM-ILD shows significant histopathologic heterogeneity that poorly correlates with HRCT patterns, particularly in anti-MDA5 positive patients who uniformly exhibited rapidly progressive ILD with diffuse alveolar damage. The major limitation of the study is that explant lungs often have extensive damage from chronic disease and infections, obscuring the original histologic pattern. Despite the limitation, these findings highlight the dynamic radiologic and histologic evolution of ILD in IIM-ILD.
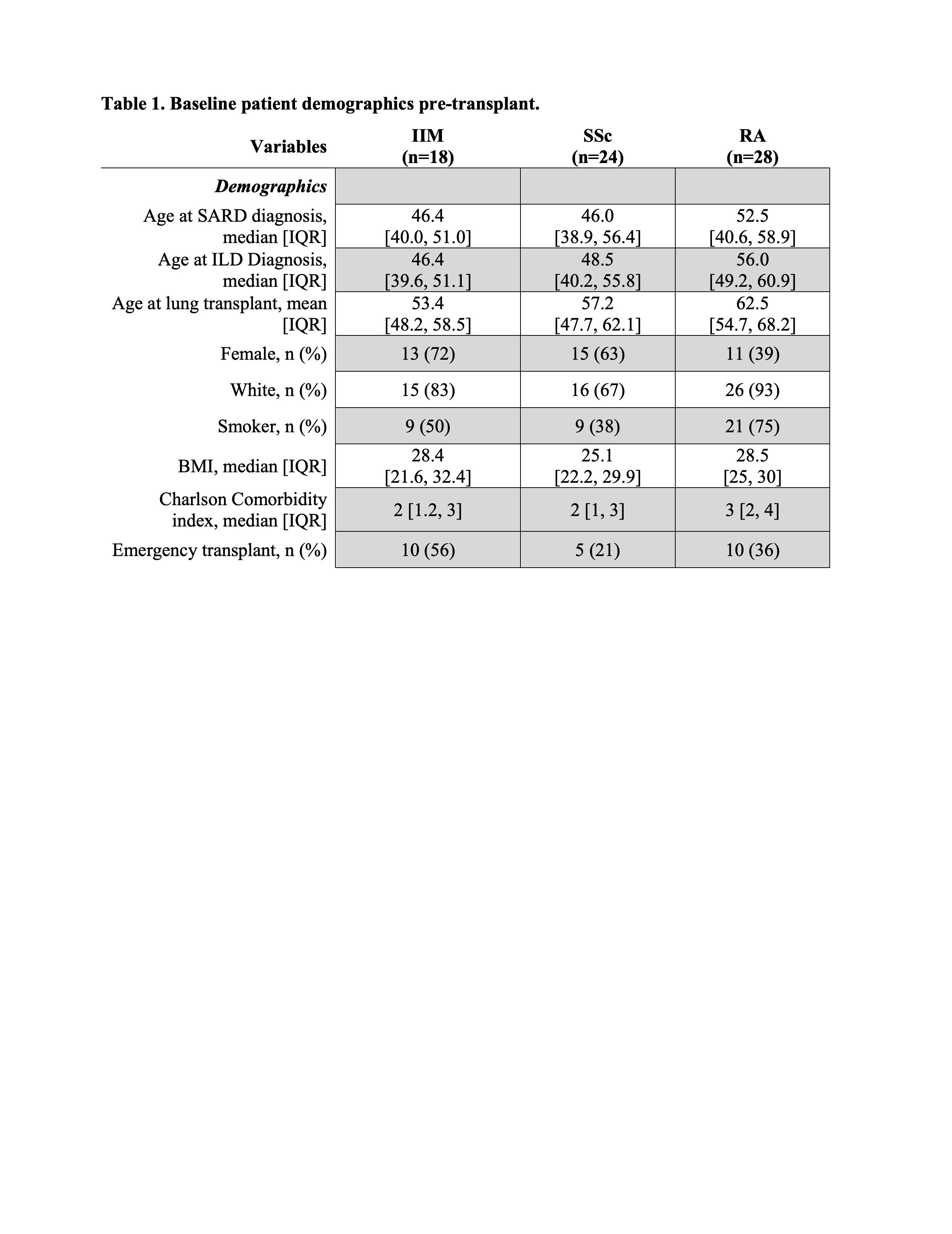 Table 1. Baseline patient demographics pre-transplant.
Table 1. Baseline patient demographics pre-transplant.
.jpg) Table 2. Radiologic pattern at ILD diagnosis and histologic findings in explanted lungs.
Table 2. Radiologic pattern at ILD diagnosis and histologic findings in explanted lungs.
.jpg) Figure 1. Alluvial chart for correlation between radiologic patterns and histopathologic findings in IIM (A), SSc (B), and RA (C).
Figure 1. Alluvial chart for correlation between radiologic patterns and histopathologic findings in IIM (A), SSc (B), and RA (C).
To cite this abstract in AMA style:
S. Jalaledin D, pye A, Chang A, Saleh N, AlHajeri S, Daviault B, Shah A, Hoa S, Landon-Cardinal O, Yu A, Levy R, Wilson J, Poirier C, Choi J, Yee J, Kim H, Huang K. Interstitial Lung Disease in Systemic Autoimmune Rheumatic Diseases (SARDs): Radiologic and Histologic Correlations [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/interstitial-lung-disease-in-systemic-autoimmune-rheumatic-diseases-sards-radiologic-and-histologic-correlations/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/interstitial-lung-disease-in-systemic-autoimmune-rheumatic-diseases-sards-radiologic-and-histologic-correlations/