Session Information
Date: Tuesday, November 14, 2023
Title: Abstracts: SLE – Diagnosis, Manifestations, & Outcomes III: Disease Activity
Session Type: Abstract Session
Session Time: 4:00PM-5:30PM
Background/Purpose: Interstitial fibrosis in lupus nephritis (LN) is often infiltrated by immune cells. However, this is typically regarded as nonspecific “scar reaction” rather than active disease requiring treatment. In contrast, scar inflammation in kidney allografts is associated with chronic rejection and treated with immunosuppression. The objective of this study was to investigate the relationship between inflammatory fibrosis and kidney disease progression in LN.
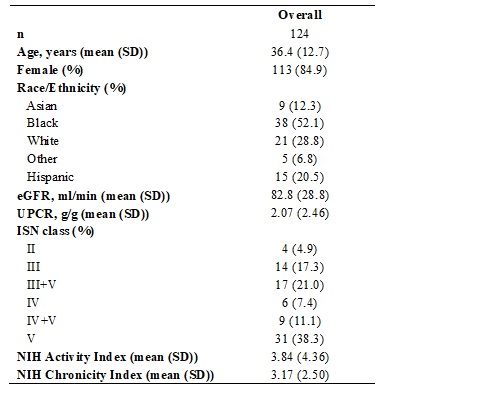
Methods: Interstitial fibrosis and tubular atrophy (IFTA) were scored in 124 kidney biopsies from patients classified as LN according to the 2018 International Society of Nephrology/Renal Pathology Society criteria. Inflammation in areas of IFTA (i-IFTA) was graded 0-3 by 2 operators and reviewed by a senior renal pathologist based on extent according to the Banff Classification of Allograft Pathology (< 10%, 10-25%, 26-50%, >50%, respectively). Glomerular filtration rate (GFR) was estimated using the CKD-EPI equation. Significant GFR loss was defined as a decline of >15 ml/min at 3 years from biopsy or end-stage kidney disease (ESKD) by year 3 requiring dialysis or transplant.
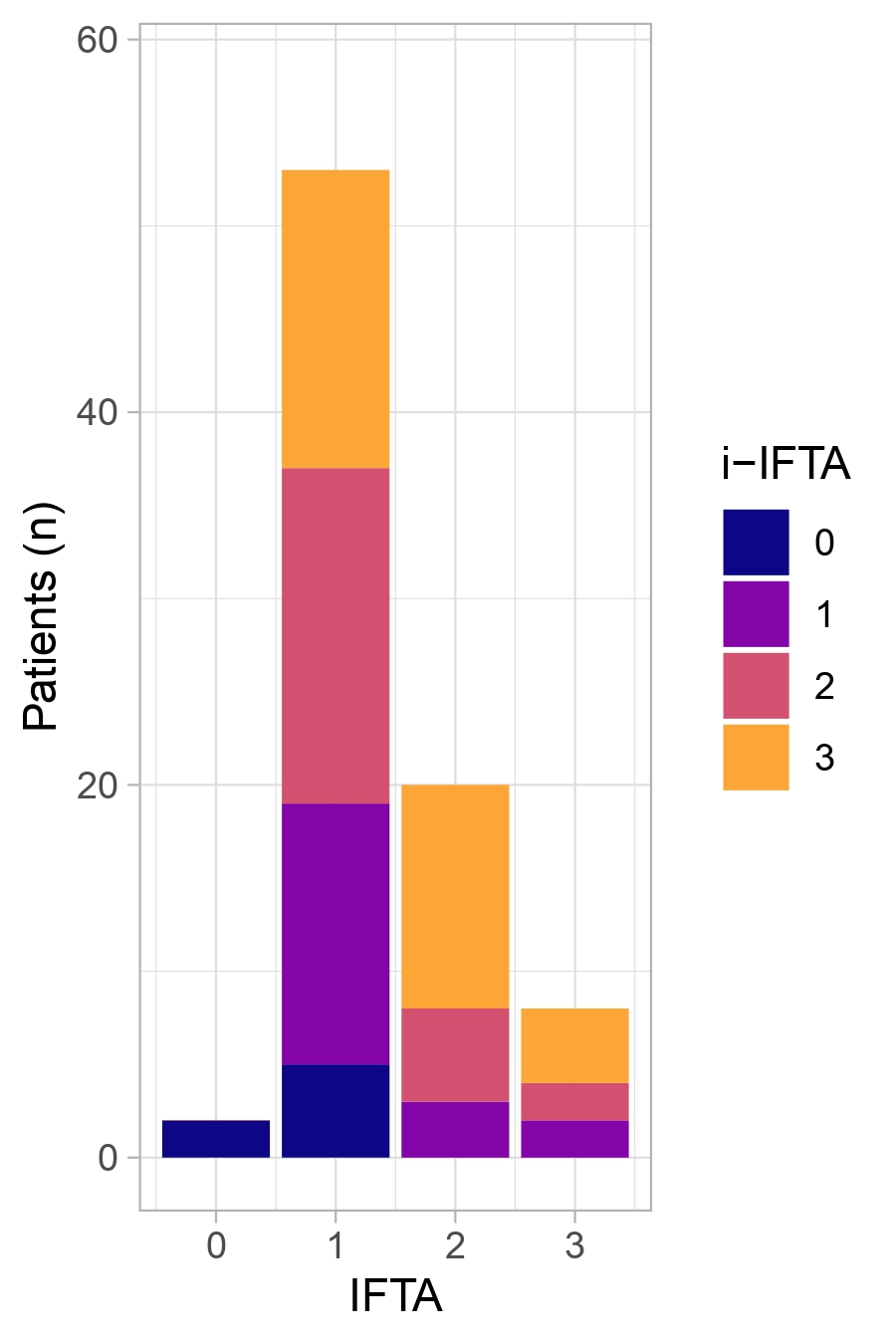
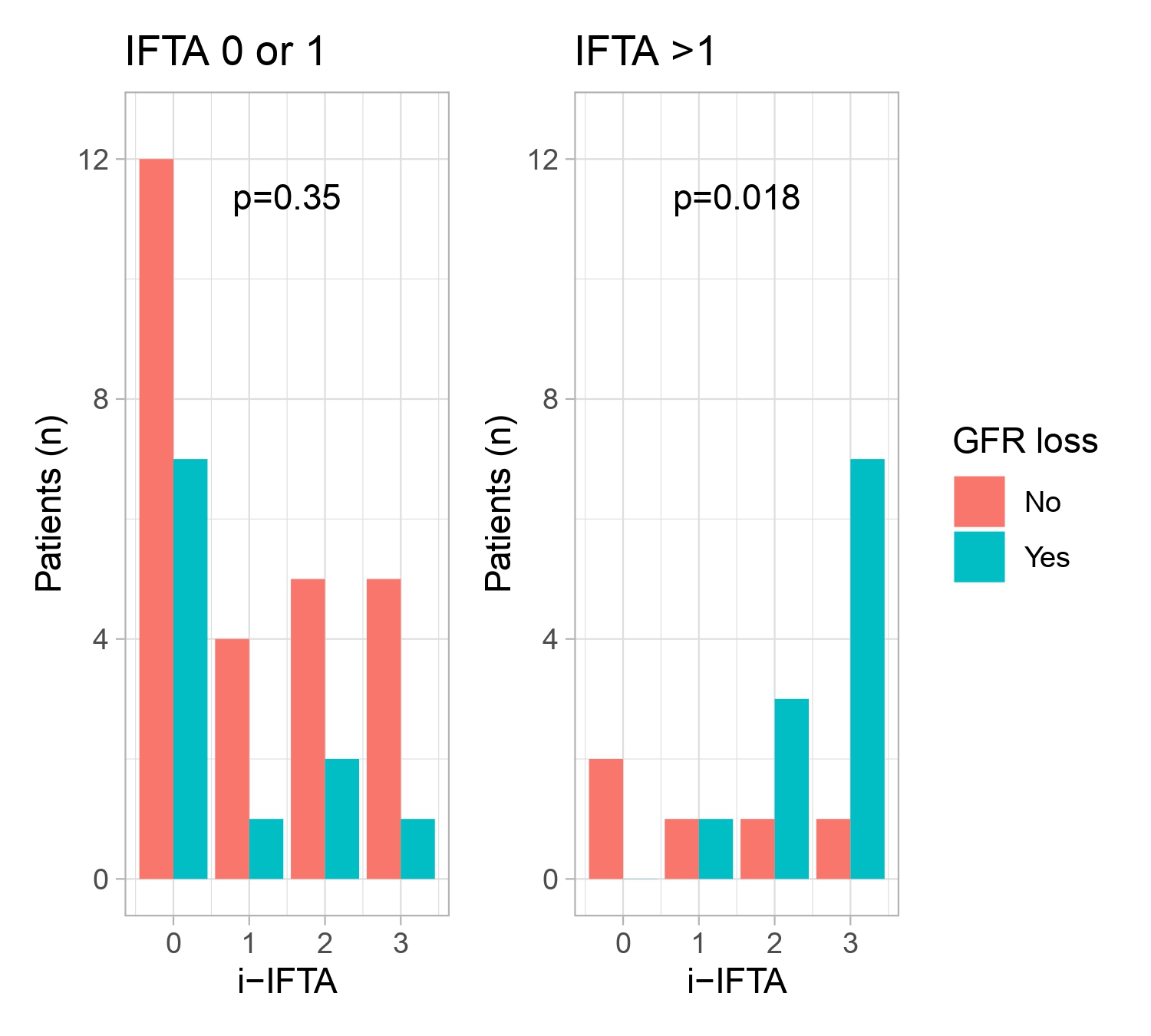
Results: The clinical and demographic characteristics of the cohort are summarized in Table 1. IFTA was observed in 88/124 (71%) biopsies, and i-IFTA was identified in 76/88 (86%) cases. The distribution of i-IFTA grades according to the degree of IFTA is illustrated in Figure 1. Of the 53 IFTA cases with 3-year follow-up data available, significant GFR loss was observed in 22/53 (42%) cases. As expected, IFTA was associated with GFR loss (p for trend = 0.03). In patients with moderate-to-severe IFTA (grade 2 or 3), the degree of i-IFTA was associated with higher risk of significant GFR loss (Figure 2). The risk of significant GFR loss in this subgroup was 0/2 (0%), 1/2 (50%), 3/4 (75%), and 7/8 (87.5%) for i-IFTA grades 0, 1, 2, and 3, respectively (p for trend = 0.018).
Conclusion: Inflammation in areas of IFTA is frequently observed in LN and exhibits substantial heterogeneity in its severity. For patients with baseline IFTA grades >1, the degree of i-IFTA emerged as a strong predictor of poor renal outcomes. These data support the routine scoring of i-IFTA in LN due to its prognostic implications and nominate i-IFTA as a potential therapeutic target.
To cite this abstract in AMA style:
Malvica S, Fenaroli P, Bagnasco S, Hodgin J, Izmirly P, Belmont H, Preisinger K, Buyon J, Magder L, Petri M, Accelerating Medicines Partnership in RA/SLE t, Rosenberg A, Fava A. Inflammatory Fibrosis Precedes Loss of Kidney Function in Lupus Nephritis [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/inflammatory-fibrosis-precedes-loss-of-kidney-function-in-lupus-nephritis/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/inflammatory-fibrosis-precedes-loss-of-kidney-function-in-lupus-nephritis/